

Shortened preoperative fasting for prevention of complications associated with laparoscopic cholecystectomy: a meta-analysis
- PMID: 28222625
- PMCID: PMC5536598
- DOI: 10.1177/0300060516676411
Shortened preoperative fasting for prevention of complications associated with laparoscopic cholecystectomy: a meta-analysis
Abstract
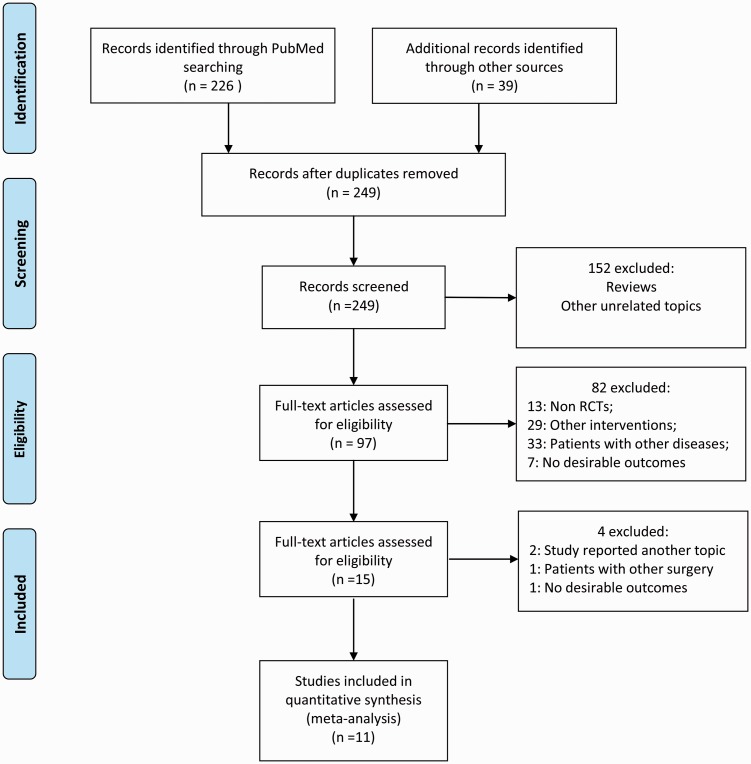
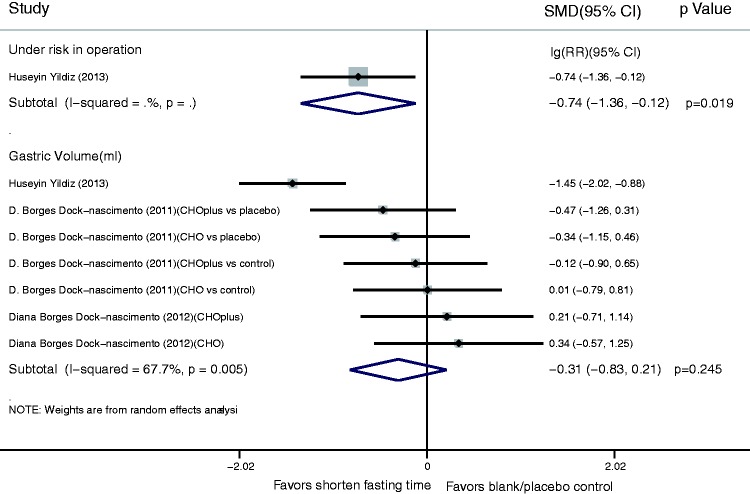
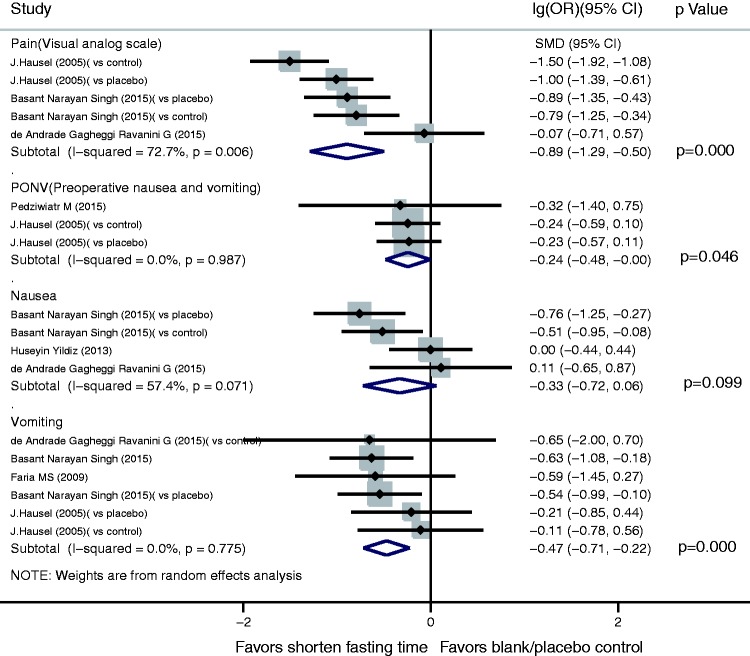
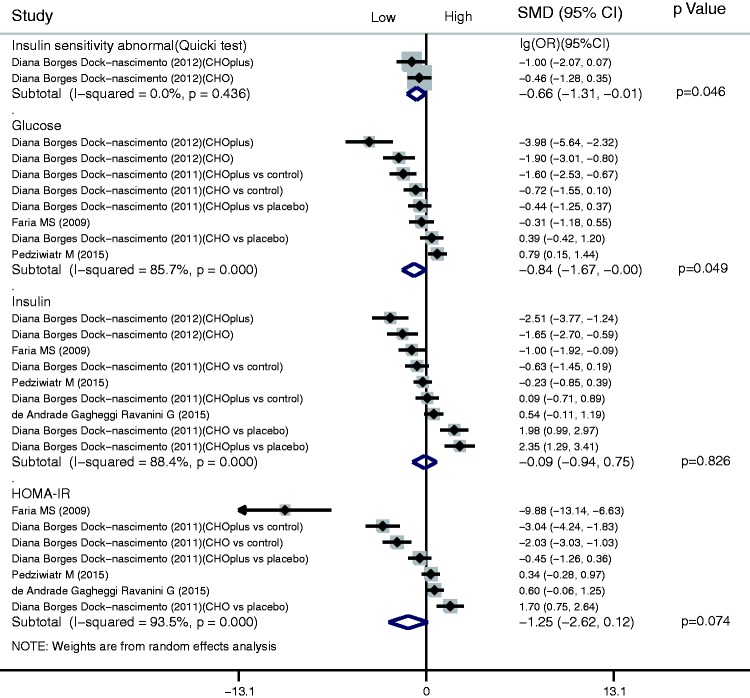
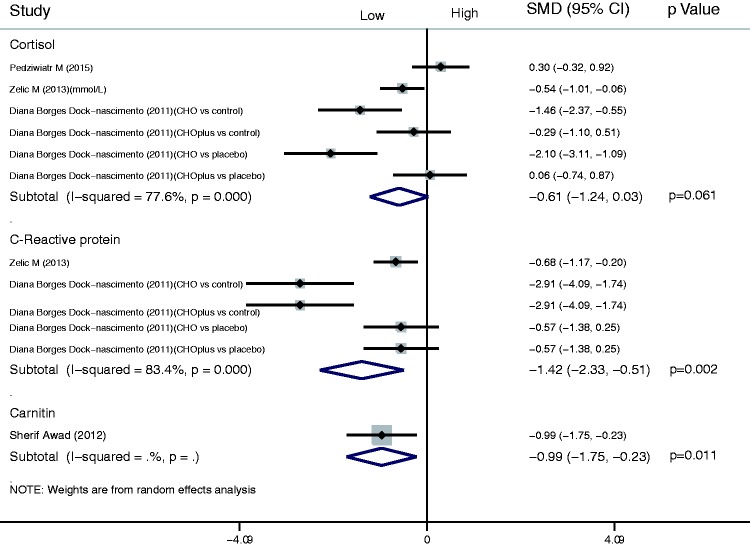
Objective Routine fasting (12 h) is always applied before laparoscopic cholecystectomy, but prolonged preoperative fasting causes thirst, hunger, and irritability as well as dehydration, low blood glucose, insulin resistance and other adverse reactions. We assessed the safety and efficacy of a shortened preoperative fasting period in patients undergoing laparoscopic cholecystectomy. Methods We searched PubMed, Embase and Cochrane Central Register of Controlled Trials up to 20 November 2015 and selected controlled trials with a shortened fasting time before laparoscopic cholecystectomy. We assessed the results by performing a meta-analysis using a variety of outcome measures and investigated the heterogeneity by subgroup analysis. Results Eleven trials were included. Forest plots showed that a shortened fasting time reduced the operative risk and patient discomfort. A shortened fasting time also reduced postoperative nausea and vomiting as well as operative vomiting. With respect to glucose metabolism, a shortened fasting time significantly reduced abnormalities in the ratio of insulin sensitivity. The C-reactive protein concentration was also reduced by a shortened fasting time. Conclusions A shortened preoperative fasting time increases patients' postoperative comfort, improves insulin resistance, and reduces stress responses. This evidence supports the clinical application of a shortened fasting time before laparoscopic cholecystectomy.
Keywords: Shortened preoperative fasting; complications; laparoscopic cholecystectomy; meta-analysis.
Figures
References
-
- Singh BN, Dahiya D, Bagaria D, et al. Effects of preoperative carbohydrates drinks on immediate postoperative outcome after day care laparoscopic cholecystectomy. Surg Endosc 2015; 29: 3267–3272. - PubMed
-
- Borges Dock-Nascimento D, Aguilar-Nascimento JE, Caporossi C, et al. Safety of oral glutamine in the abbreviation of preoperative fasting: a double-blind, controlled, randomized clinical trial. Nutr Hosp 2011; 26: 86–90. - PubMed
-
- Pędziwiatr M, Pisarska M, Matłok M, et al. Randomized clinical trial to compare the effects of preoperative oral carbohydrate loading versus placebo on insulin resistance and cortisol level after laparoscopic cholecystectomy. Pol Przegl Chir 2015; 87: 402–408. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
