

Birt-Hogg-Dubé syndrome: a literature review and case study of a Chinese woman presenting a novel FLCN mutation
- PMID: 28222720
- PMCID: PMC5320703
- DOI: 10.1186/s12890-017-0383-9
Birt-Hogg-Dubé syndrome: a literature review and case study of a Chinese woman presenting a novel FLCN mutation
Abstract
Background: The Birt-Hogg-Dubé (BHD) syndrome is a very rare autosomal dominant form of genodermatosis caused by germline mutations in the folliculin (FLCN) gene, which is mapped to the p11.2 region in chromosome 17. BHD commonly presents cutaneous fibrofolliculomas, pulmonary cysts, renal cell carcinoma, and recurrent pneumothoraxes. The disease is easily ignored or misdiagnosed as pneumothorax, pulmonary lymphangiomyomatosis (LAM), or emphysema. Follow-up and guidelines for managing recurrent pneumothoraxes in these patients are lacking.
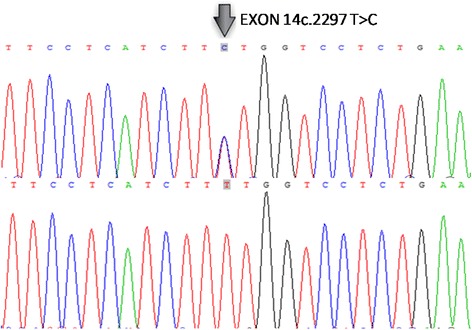
Case presentation: We reported the case of a 56-year-old Chinese woman who presented skin lesions, multiple lung bubblae, recurrent pneumothoraxes, thyroid nodules, and pulmonary inflammatory pseudotumors (PITs). The patient had a family history of pneumothoraxes and renal tumor. The BHD diagnosis was confirmed by genetic testing, which revealed a novel FLCN mutation in exon 14. Furthermore, the patient underwent a bullectomy because of recurrent pneumothorax 6 years ago.
Conclusion: To our knowledge, the novel mutation in exon 14 and the manifestation of PIT in the present case have never been reported for BHD. The patient underwent a bullectomy previously with no relapse at the last follow-up before the preparation of this report, thereby suggesting that thoracotomy with bullectomy may be a possible therapeutic approach for some BHD patients with recurrent pneumothorax.
Keywords: Birt–Hogg–Dubé syndrome; Lung bubblae; Mutation; Pneumothorax; Treatment.
Figures


Similar articles
-
Birt-Hogg-Dubé syndrome in Korean: clinicoradiologic features and long term follow-up.Korean J Intern Med. 2019 Jul;34(4):830-840. doi: 10.3904/kjim.2018.119. Epub 2018 Oct 26. Korean J Intern Med. 2019. PMID: 30360018 Free PMC article.
-
Novel germline mutations in FLCN gene identified in two Chinese patients with Birt-Hogg-Dubé syndrome.Chin J Cancer. 2017 Jan 9;36(1):4. doi: 10.1186/s40880-016-0172-5. Chin J Cancer. 2017. PMID: 28069055 Free PMC article.
-
A Case of Birt-Hogg-Dubé (BHD) Syndrome Harboring a Novel Folliculin (FLCN) Gene Mutation.Am J Case Rep. 2016 Oct 26;17:788-792. doi: 10.12659/ajcr.899407. Am J Case Rep. 2016. PMID: 27780965 Free PMC article.
-
Birt-Hogg-Dubé Syndrome.Clin Chest Med. 2016 Sep;37(3):475-86. doi: 10.1016/j.ccm.2016.04.010. Epub 2016 Jun 25. Clin Chest Med. 2016. PMID: 27514594 Review.
-
Birt-Hogg-Dubé Syndrome: A Review of Dermatological Manifestations and Other Symptoms.Am J Clin Dermatol. 2018 Feb;19(1):87-101. doi: 10.1007/s40257-017-0307-8. Am J Clin Dermatol. 2018. PMID: 28695430 Review.
Cited by
-
Birt-Hogg-Dubé syndrome in Chinese patients: a literature review of 120 families.Orphanet J Rare Dis. 2021 May 17;16(1):223. doi: 10.1186/s13023-021-01848-8. Orphanet J Rare Dis. 2021. PMID: 34001170 Free PMC article. Review.
-
The clinical characteristics of East Asian patients with Birt-Hogg-Dubé syndrome.Ann Transl Med. 2020 Nov;8(21):1436. doi: 10.21037/atm-20-1129. Ann Transl Med. 2020. PMID: 33313181 Free PMC article.
-
Birt-Hogg-Dubé syndrome - a rare genetic disorder complicated by pneumothorax: A case report.World J Clin Cases. 2025 Jun 26;13(18):100610. doi: 10.12998/wjcc.v13.i18.100610. World J Clin Cases. 2025. PMID: 40574922 Free PMC article.
-
Clinical and Genetic Comparison of Birt-Hogg-Dubé Syndrome (Hornstein-Knickenberg Syndrome) in Chinese: A Systemic Review of Reported Cases.Int J Gen Med. 2022 May 23;15:5111-5121. doi: 10.2147/IJGM.S359660. eCollection 2022. Int J Gen Med. 2022. PMID: 35637701 Free PMC article. Review.
References
-
- Nahorski MS, Lim DH, Martin L, Gille JJ, McKay K, Rehal PK, Ploeger HM, van Steensel M, Tomlinson IP, Latif F, et al. Investigation of the Birt-Hogg-Dube tumour suppressor gene (FLCN) in familial and sporadic colorectal cancer. J Med Genet. 2010;47(6):385–90. doi: 10.1136/jmg.2009.073304. - DOI - PubMed
-
- Toro JR, Wei MH, Glenn GM, Weinreich M, Toure O, Vocke C, Turner M, Choyke P, Merino MJ, Pinto PA, et al. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dube syndrome: a new series of 50 families and a review of published reports. J Med Genet. 2008;45(6):321–31. doi: 10.1136/jmg.2007.054304. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
