

Increases in IgE, Eosinophils, and Mast Cells Can be Used in Diagnosis and to Predict Relapse of IgG4-Related Disease
- PMID: 28223204
- PMCID: PMC5592233
- DOI: 10.1016/j.cgh.2017.02.007
Increases in IgE, Eosinophils, and Mast Cells Can be Used in Diagnosis and to Predict Relapse of IgG4-Related Disease
Abstract
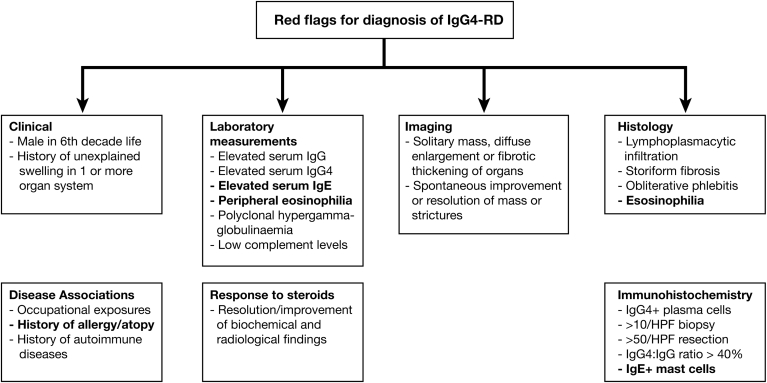
Background & aims: IgG subclass 4-related disease (IgG4-RD) is characterized by increased serum levels of IgG4 and infiltration of biliary, pancreatic, and other tissues by IgG4-positive plasma cells. We assessed the prevalence of allergy and/or atopy, serum, and tissue IgE antibodies, and blood and tissue eosinophils in patients with IgG4-RD. We investigated the association between serum IgE and diagnosis and relapse of this disease.
Methods: We performed a prospective study of 48 patients with IgG4-RD, 42 patients with an increased serum level of IgG4 with other inflammatory and autoimmune conditions (disease control subjects), and 51 healthy individuals (healthy control subjects) recruited from Oxford, United Kingdom from March 2010 through March 2014, and followed for a median of 41 months (range, 3-73 months). Serum levels of immunoglobulin were measured at diagnosis, during steroid treatment, and at disease relapse for patients with IgG4-RD; levels at diagnosis were compared with baseline levels of control subjects. Allergen-specific IgEs were measured using the IgE ImmunoCAP. Levels and distribution of IgG4 and IgE antibodies in lymphoid, biliary, and pancreatic tissues from patients with IgG4-RD and disease control subjects were measured by immunohistochemistry. We analyzed data using the Spearman rank correlation and receiver operating characteristic curves.
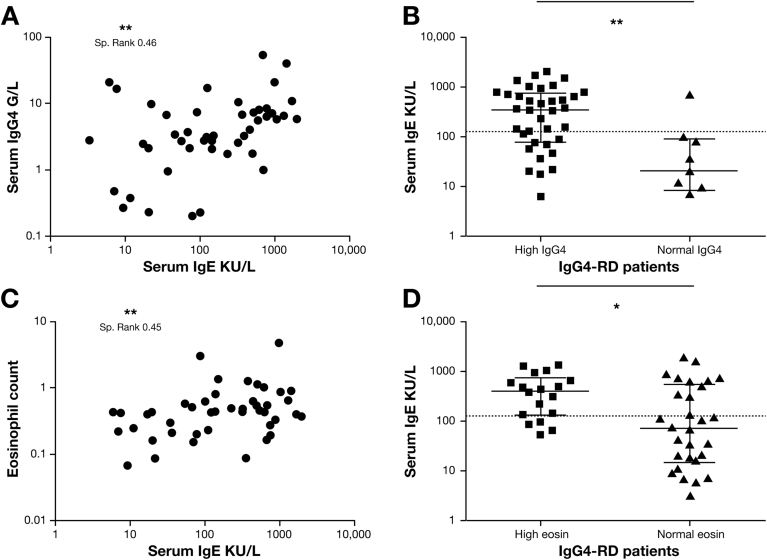
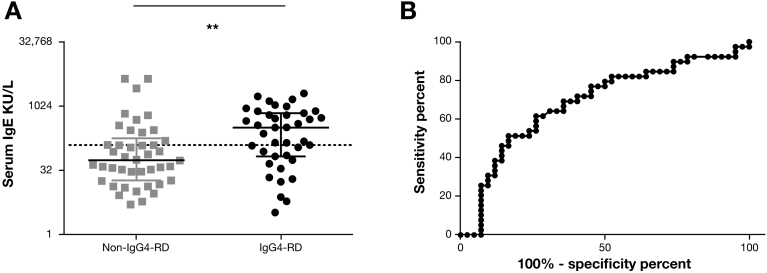
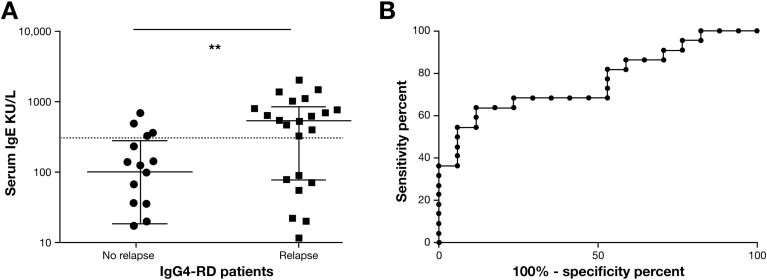
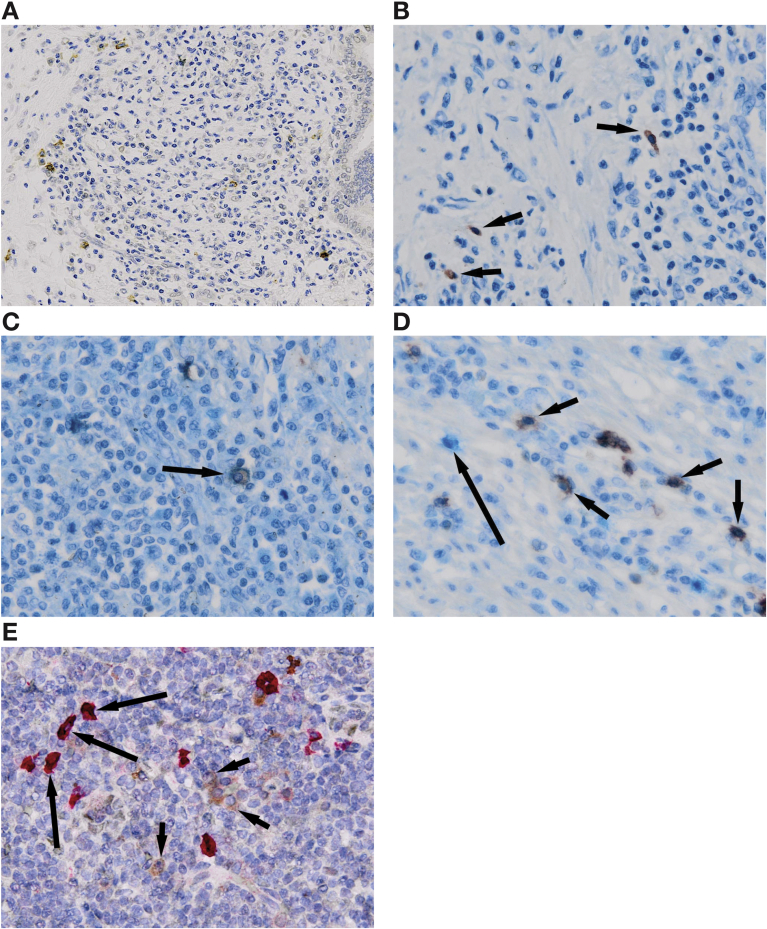
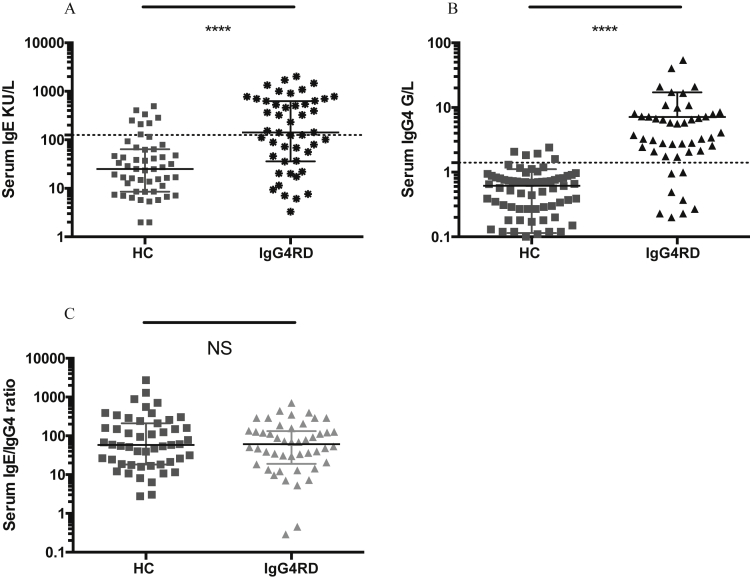
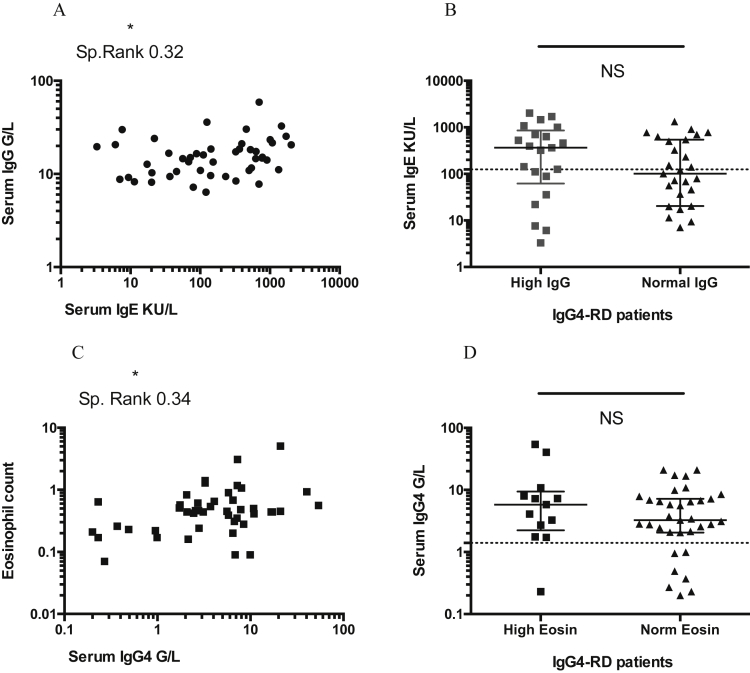
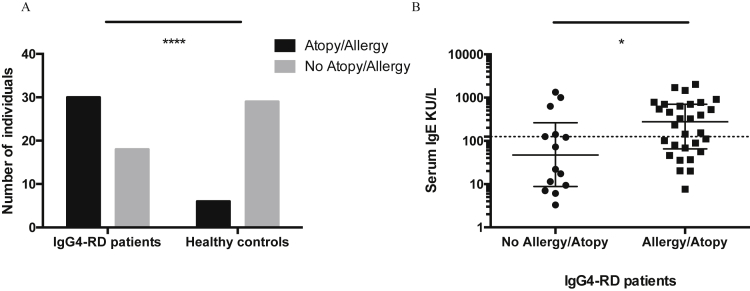
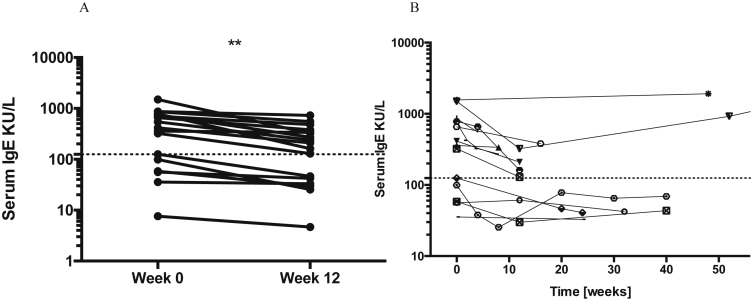
Results: Serum levels of IgG4 increased to 1.4 g/L or more, and IgE increased to 125 kIU/L or more, in 81% and 54% of patients with IgG4-RD, respectively, compared with 6% and 16% of healthy control subjects (P < .0001). Peripheral blood eosinophilia was detected in 38% of patients with IgG4-RD versus 9% of healthy control subjects (P = .004). Of patients with IgG4-RD, 63% had a history of allergy and 40% had a history of atopy with an IgE-specific response; these values were 60% and 53% in patients with increased serum levels of IgE (P < .05). Level of IgE at diagnosis >480 kIU/L distinguished patients with IgG4-RD from disease control subjects with 86% specificity, 36% sensitivity, and a likelihood ratio of 3.2. Level of IgE at diagnosis >380 kIU/L identified patients with disease relapse with 88% specificity, 64% sensitivity, and a likelihood ratio of 5.4. IgE-positive mast cells and eosinophilia were observed in lymphoid, biliary, and pancreatic tissue samples from 50% and 86% of patients with IgG4-RD, respectively.
Conclusions: In a prospective study, we associated IgG4-RD with allergy, atopy, eosinophilia, increased serum levels of IgE, and IgE-positive mast cells in lymphoid, biliary, and pancreatic tissue. An IgE-mediated allergic response therefore seems to develop in most patients with IgG4-RD; levels of IgE might be used in diagnosis and predicting relapse.
Keywords: Detection; Immune Response; Inflammation; Pancreas.
Copyright © 2017 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Deshpande V., Zen Y., Chan J.K. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25:1181–1192. - PubMed
-
- Kamisawa T., Anjiki H., Egawa N. Allergic manifestations in autoimmune pancreatitis. Eur J Gastroenterol Hepatol. 2009;21:1136–1139. - PubMed
-
- Sah R.P., Pannala R., Chari S.T. Prevalence, diagnosis, and profile of autoimmune pancreatitis presenting with features of acute or chronic pancreatitis. Clin Gastroenterol Hepatol. 2010;8:91–96. - PubMed
-
- Umemura T., Zen Y., Hamano H. Immunoglobin G4-hepatopathy: association of immunoglobin G4-bearing plasma cells in liver with autoimmune pancreatitis. Hepatology. 2007;46:463–471. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
