

Assessment of liver iron overload by 3 T MRI
- PMID: 28224171
- PMCID: PMC6437287
- DOI: 10.1007/s00261-017-1077-8
Assessment of liver iron overload by 3 T MRI
Abstract
Purpose: To evaluate the performance and limitations of the signal intensity ratio method for quantifying liver iron overload at 3 T.
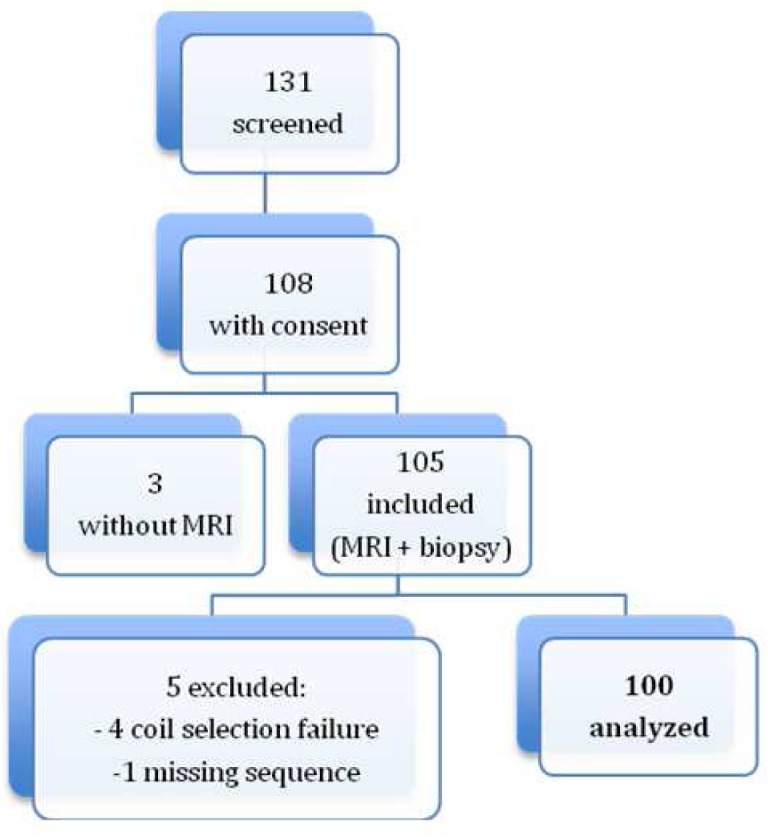
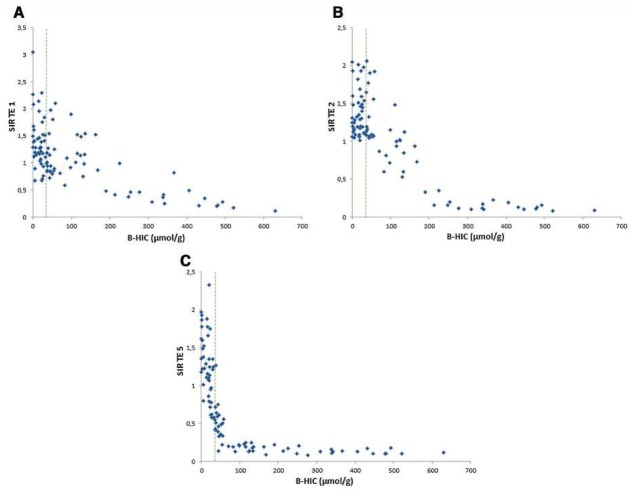
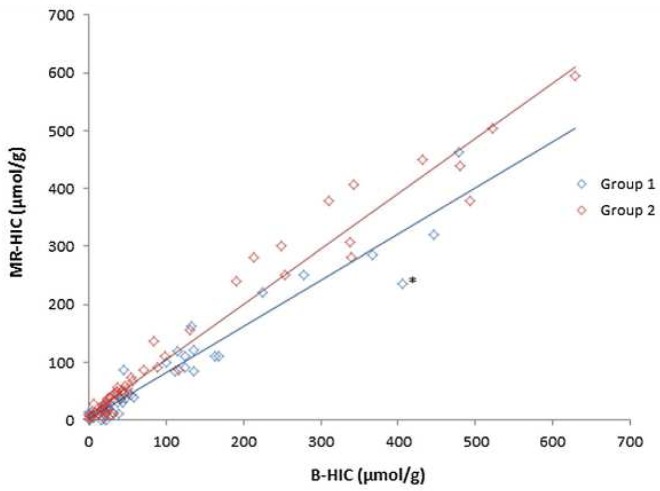
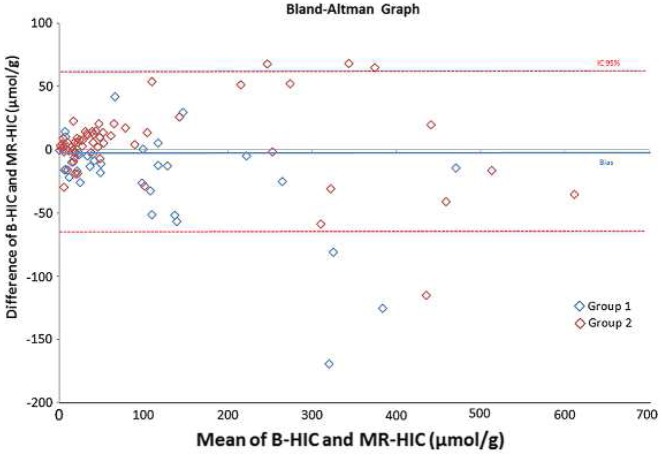
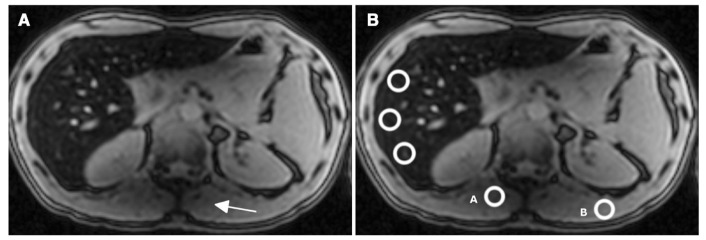
Methods: Institutional review board approval and written informed consent from all participants were obtained. One hundred and five patients were included prospectively. All patients underwent a liver biopsy with biochemical assessment of hepatic iron concentration and a 3 T MRI scan with 5 breath-hold single-echo gradient-echo sequences. Linear correlation between liver-to-muscle signal intensity ratio and liver iron concentration was calculated. The algorithm for calculating magnetic resonance hepatic iron concentration was adapted from the method described by Gandon et al. with echo times divided by 2. Sensitivity and specificity were calculated.
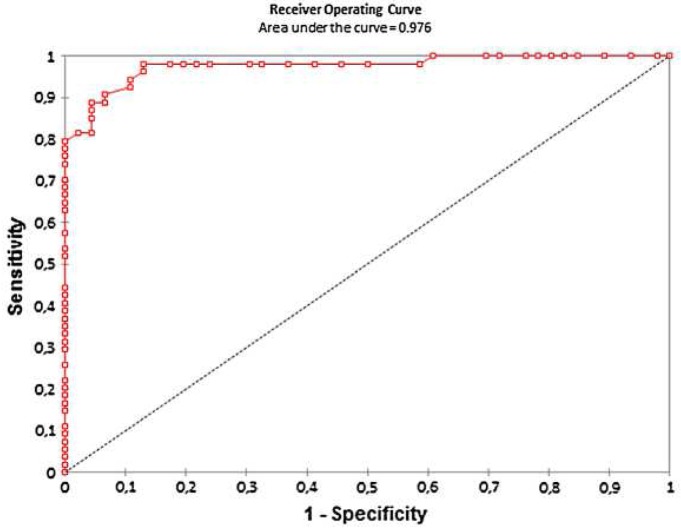
Results: Five patients were excluded (coil selection failure or missing sequence) and 100 patients were analyzed, 64 men and 36 women, 52 ± 13.3 years old, with a biochemical hepatic iron concentration range of 0-630 µmol/g. Linear correlation between biochemical hepatic iron concentration and MR-hepatic iron concentration was excellent with a correlation coefficient = 0.96, p < 0.0001. Sensitivity and specificity were, respectively, 83% (0.70-0.92) and 96% (0.85-0.99), with a pathological threshold of 36 µmol/g.
Conclusion: Signal intensity ratio method for quantifying liver iron overload can be used at 3 T with echo times divided by 2.
Keywords: 3 Tesla; Iron overload; Liver; MRI; Quantification.
Figures
References
-
- Deugnier Y, Turlin B. Iron and hepatocellular carcinoma. J Gastroenterol Hepatol. 2001;16:491–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
