

Clinical characteristics and outcome of Spanish patients with ANCA-associated vasculitides: Impact of the vasculitis type, ANCA specificity, and treatment on mortality and morbidity
- PMID: 28225490
- PMCID: PMC5569416
- DOI: 10.1097/MD.0000000000006083
Clinical characteristics and outcome of Spanish patients with ANCA-associated vasculitides: Impact of the vasculitis type, ANCA specificity, and treatment on mortality and morbidity
Abstract
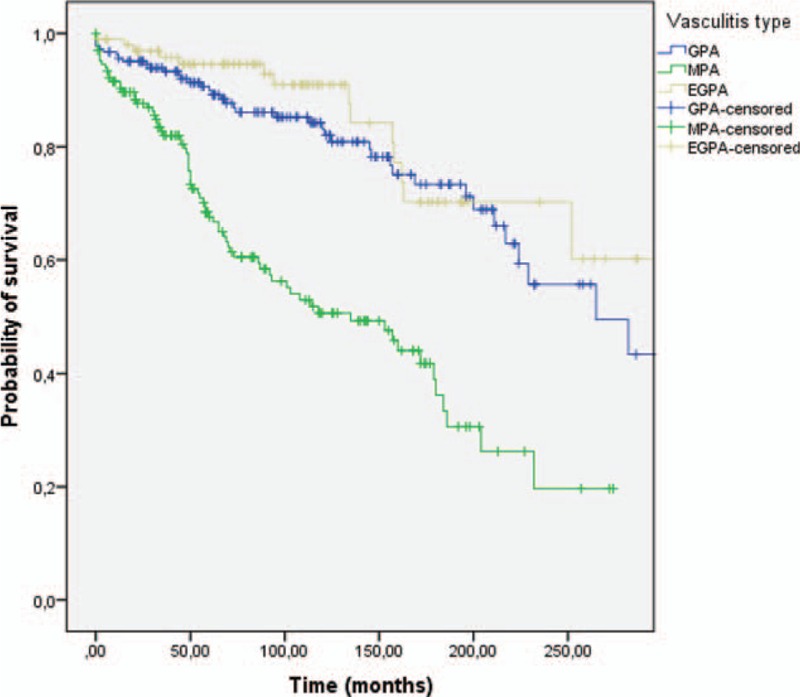
The aim of this study was to describe the clinical characteristics of ANCA-associated vasculitides (AAV) at presentation, in a wide cohort of Spanish patients, and to analyze the impact of the vasculitis type, ANCA specificity, prognostic factors, and treatments administered at diagnosis, in the outcome.A total of 450 patients diagnosed between January 1990 and January 2014 in 20 Hospitals from Spain were included. Altogether, 40.9% had granulomatosis with polyangiitis (GPA), 37.1% microscopic polyangiitis (MPA), and 22% eosinophilic granulomatosis with polyangiitis (EGPA). The mean age at diagnosis was 55.6 ± 17.3 years, patients with MPA being significantly older (P < 0.001). Fever, arthralgia, weight loss, respiratory, and ear-nose-throat (ENT) symptoms, were the most common at disease onset. ANCAs tested positive in 86.4% of cases: 36.2% C-ANCA-PR3 and 50.2% P-ANCA-MPO. P-ANCA-MPO was significantly associated with an increased risk for renal disease (OR 2.6, P < 0.001) and alveolar hemorrhage (OR 2, P = 0.010), while C-ANCA-PR3 was significantly associated with an increased risk for ENT (OR 3.4, P < 0.001) and ocular involvement (OR 2.3, P = 0.002). All patients received corticosteroids (CS) and 74.9% cyclophosphamide (CYC). The median follow-up was 82 months (IQR 100.4). Over this period 39.9% of patients suffered bacterial infections and 14.6% opportunistic infections, both being most prevalent in patients with high-cumulated doses of CYC and CS (P < 0.001). Relapses were recorded in 36.4% of cases with a mean rate of 2.5 ± 2.3, and were more frequent in patients with C-ANCA-PR3 (P = 0.012). The initial disease severity was significantly associated with mortality but not with the occurrence of relapses. One hundred twenty-nine (28.7%) patients (74 MPA, 41 GPA, 14 EGPA) died. The mean survival was 58 months (IQR 105) and was significantly lower for patients with MPA (P < 0.001). Factors independently related to death were renal involvement (P = 0.010), cardiac failure (P = 0.029) and age over 65 years old (P < 0.001) at disease onset, and bacterial infections (P < 0.001). An improved outcome with significant decrease in mortality and treatment-related morbidity was observed in patients diagnosed after 2000, and was related to the implementation of less toxic regimens adapted to the disease activity and stage, and a drastic reduction in the cumulated CYC and CS dose.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Leavitt RY, Fauci AS, Bloch DA, et al. The American College of Rheumatology criteria for the classification of Wegener's Granulomatosis. Arthritis Rheum 1990;33:1101–7. - PubMed
-
- Masi AT, Hunder GG, Lie JT, et al. The American college of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (Allergic granulomatosis and angiitis). Arthritis Rheum 1990;33:1094–100. - PubMed
-
- Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 2013;65:1–1. - PubMed
-
- Fauci AS, Haynes BF, Katz P, et al. Wegener's granulomatosis: prospective clinical and therapeutic experience with 85 patients for 21 years. Ann Intern Med 1983;98:76–85. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
