

Loss of PTEN Is Associated with Resistance to Anti-PD-1 Checkpoint Blockade Therapy in Metastatic Uterine Leiomyosarcoma
- PMID: 28228279
- PMCID: PMC5408320
- DOI: 10.1016/j.immuni.2017.02.001
Loss of PTEN Is Associated with Resistance to Anti-PD-1 Checkpoint Blockade Therapy in Metastatic Uterine Leiomyosarcoma
Abstract
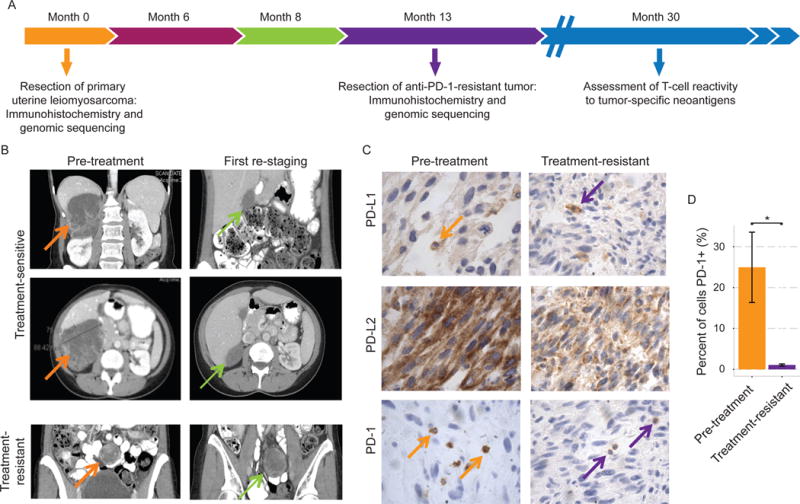
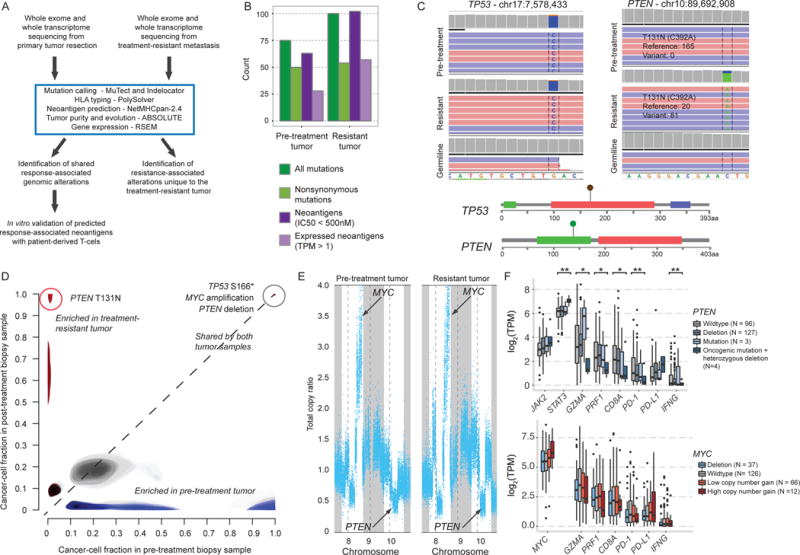
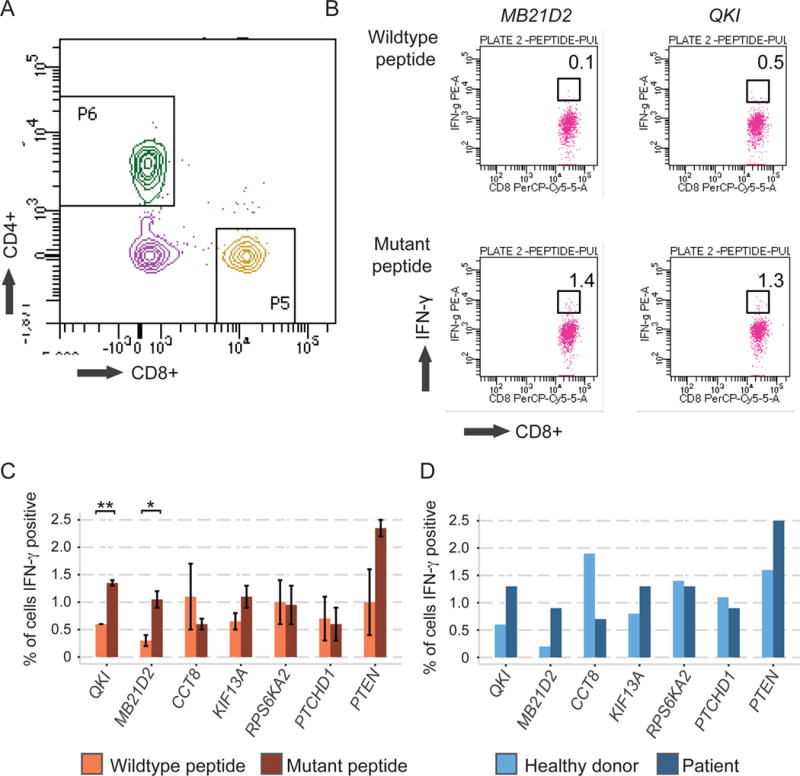
Response to immune checkpoint blockade in mesenchymal tumors is poorly characterized, but immunogenomic dissection of these cancers could inform immunotherapy mediators. We identified a treatment-naive patient who has metastatic uterine leiomyosarcoma and has experienced complete tumor remission for >2 years on anti-PD-1 (pembrolizumab) monotherapy. We analyzed the primary tumor, the sole treatment-resistant metastasis, and germline tissue to explore mechanisms of immunotherapy sensitivity and resistance. Both tumors stained diffusely for PD-L2 and showed sparse PD-L1 staining. PD-1+ cell infiltration significantly decreased in the resistant tumor (p = 0.039). Genomically, the treatment-resistant tumor uniquely harbored biallelic PTEN loss and had reduced expression of two neoantigens that demonstrated strong immunoreactivity with patient T cells in vitro, suggesting long-lasting immunological memory. In this near-complete response to PD-1 blockade in a mesenchymal tumor, we identified PTEN mutations and reduced expression of genes encoding neoantigens as potential mediators of resistance to immune checkpoint therapy.
Keywords: exceptional response; immune checkpoint; immunotherapy; neoantigen; sarcoma; whole-exome sequencing; whole-transcriptome sequencing.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
