

Neighborhood Differences in Post-Stroke Mortality
- PMID: 28228449
- PMCID: PMC5328121
- DOI: 10.1161/CIRCOUTCOMES.116.002547
Neighborhood Differences in Post-Stroke Mortality
Abstract
Background: Post-stroke mortality is higher among residents of disadvantaged neighborhoods, but it is not known whether neighborhood inequalities are specific to stroke survival or similar to mortality patterns in the general population. We hypothesized that neighborhood disadvantage would predict higher poststroke mortality, and neighborhood effects would be relatively larger for stroke patients than for individuals with no history of stroke.
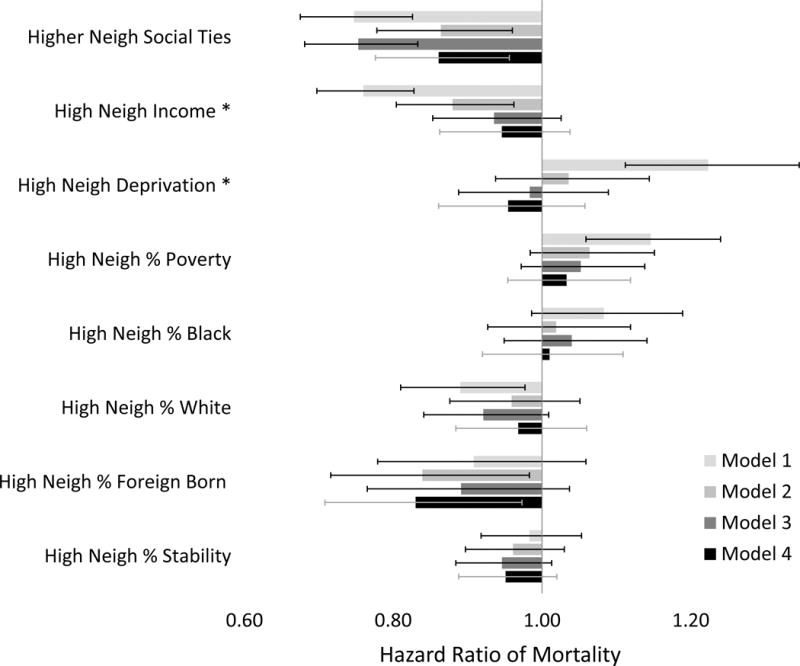
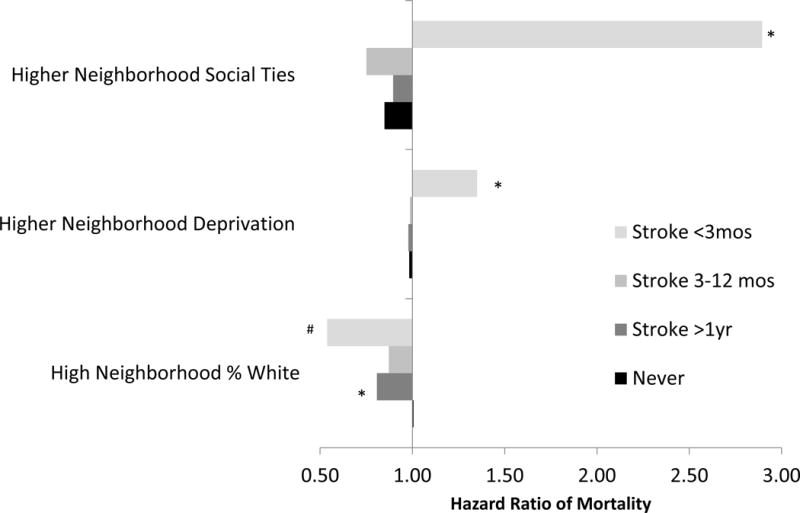
Methods and results: Health and Retirement Study participants aged ≥50 years without stroke at baseline (n=15 560) were followed ≤12 years for incident stroke (1715 events over 159 286 person-years) and mortality (5325 deaths). Baseline neighborhood characteristics included objective measures based on census tracts (family income, poverty, deprivation, residential stability, and percent white, black, or foreign-born) and self-reported neighborhood social ties. Using Cox proportional hazard models, we compared neighborhood mortality effects for people with versus people without a history of stroke. Most neighborhood variables predicted mortality for both stroke patients and the general population in demographic-adjusted models. Neighborhood percent white predicted lower mortality for stroke survivors (hazard ratio, 0.75 for neighborhoods in highest 25th percentile versus below, 95% confidence interval, 0.62-0.91) more strongly than for stroke-free adults (hazard ratio, 0.92; 95% confidence interval, 0.83-1.02; P=0.04 for stroke-by-neighborhood interaction). No other neighborhood characteristic had different effects for people with versus without stroke. Neighborhood-mortality associations emerged within 3 months after stroke, when associations were often stronger than among stroke-free individuals.
Conclusions: Neighborhood characteristics predict mortality, but most effects are similar for individuals without stroke. Eliminating disparities in stroke survival may require addressing pathways that are not specific to traditional poststroke care.
Keywords: community; mortality; neighborhood; social support; socioeconomic factors; stroke.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Lackland DT, Roccella EJ, Deutsch AF, Fornage M, George MG, Howard G, Kissela BM, Kittner SJ, Lichtman JH, Lisabeth LD, Schwamm LH, Smith EE, Towfighi A. Factors influencing the decline in stroke mortality: A statement from the american heart association/american stroke association. Stroke. 2014;45:315–353. - PMC - PubMed
-
- Thrift AG, Dewey HM, Sturm JW, Paul SL, Gilligan AK, Srikanth VK, Macdonell RAL, McNeil JJ, Macleod MR, Donnan GA. Greater incidence of both fatal and nonfatal strokes in disadvantaged areas: The northeast melbourne stroke incidence study. Stroke. 2006;37:877–882. - PubMed
-
- Menec VH, Shooshtari S, Nowicki S, Fournier S. Does the relationship between neighborhood socioeconomic status and health outcomes persist into very old age? A population-based study. J Aging Health. 2010;22:27–47. - PubMed
-
- Brown P, Guy M, Broad J. Individual socio-economic status, community socio-economic status and stroke in new zealand: A case control study. Soc Sci Med. 2005;61:1174–1188. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
