

Prognostic Value of Residual Urine Volume, GFR by 24-hour Urine Collection, and eGFR in Patients Receiving Dialysis
- PMID: 28228465
- PMCID: PMC5338702
- DOI: 10.2215/CJN.05520516
Prognostic Value of Residual Urine Volume, GFR by 24-hour Urine Collection, and eGFR in Patients Receiving Dialysis
Abstract
Background and objectives: Residual kidney function can be assessed by simply measuring urine volume, calculating GFR using 24-hour urine collection, or estimating GFR using the proposed equation (eGFR). We aimed to investigate the relative prognostic value of these residual kidney function parameters in patients on dialysis.
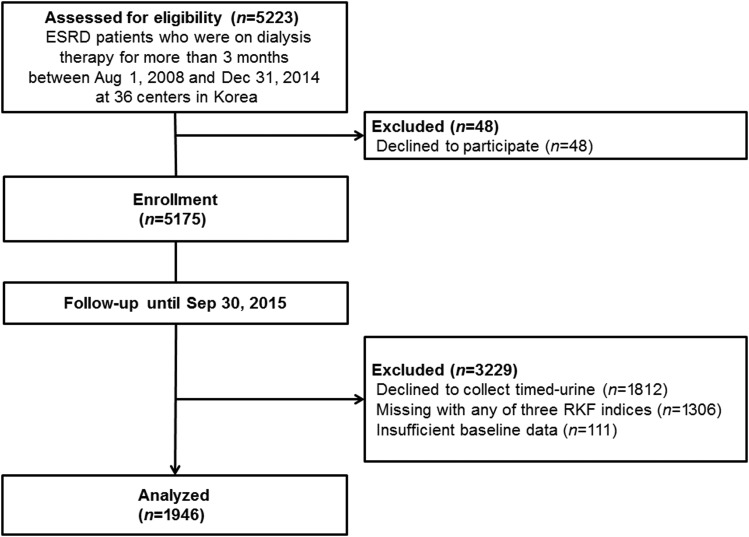
Design, setting, participants, & measurements: Using the database from a nationwide prospective cohort study, we compared differential implications of the residual kidney function indices in 1946 patients on dialysis at 36 dialysis centers in Korea between August 1, 2008 and December 31, 2014. Residual GFR calculated using 24-hour urine collection was determined by an average of renal urea and creatinine clearance on the basis of 24-hour urine collection. eGFR-urea, creatinine and eGFR β2-microglobulin were calculated from the equations using serum urea and creatinine and β2-microglobulin, respectively. The primary outcome was all-cause death.
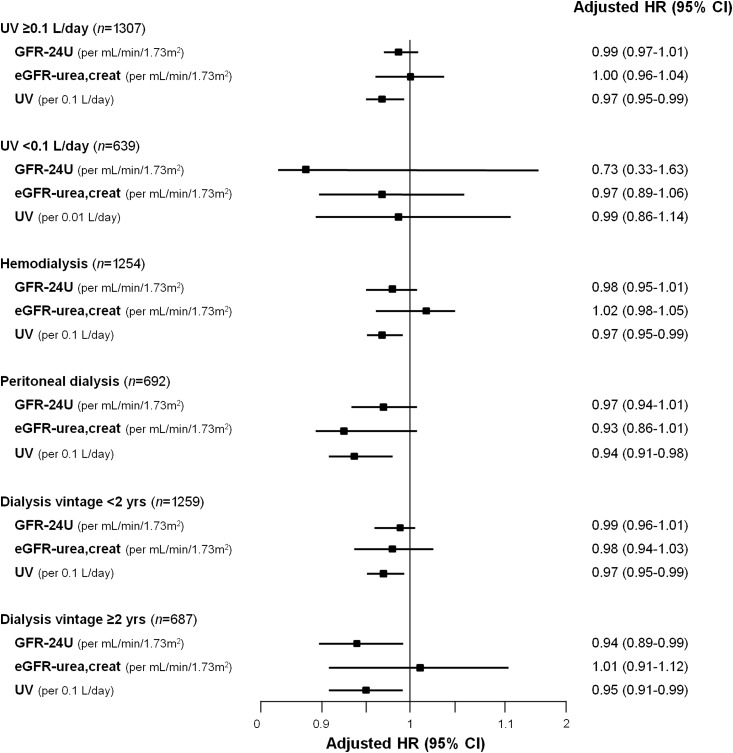
Results: During a mean follow-up of 42 months, 385 (19.8%) patients died. In multivariable Cox analyses, residual urine volume (hazard ratio, 0.96 per 0.1-L/d higher volume; 95% confidence interval, 0.94 to 0.98) and GFR calculated using 24-hour urine collection (hazard ratio, 0.98; 95% confidence interval, 0.95 to 0.99) were independently associated with all-cause mortality. In 1640 patients who had eGFR β2-microglobulin data, eGFR β2-microglobulin (hazard ratio, 0.98; 95% confidence interval, 0.96 to 0.99) was also significantly associated with all-cause mortality as well as residual urine volume (hazard ratio, 0.96 per 0.1-L/d higher volume; 95% confidence interval, 0.94 to 0.98) and GFR calculated using 24-hour urine collection (hazard ratio, 0.97; 95% confidence interval, 0.95 to 0.99). When each residual kidney function index was added to the base model, only urine volume improved the predictability for all-cause mortality (net reclassification index =0.11, P=0.01; integrated discrimination improvement =0.01, P=0.01).
Conclusions: Higher residual urine volume was significantly associated with a lower risk of death and exhibited a stronger association with mortality than GFR calculated using 24-hour urine collection and eGFR-urea, creatinine. These results suggest that determining residual urine volume may be beneficial to predict patient survival in patients on dialysis.
Keywords: dialysis; end-stage renal disease; glomerular filtration rate; mortality; residual kidney function; urine volume.
Copyright © 2017 by the American Society of Nephrology.
Figures
Comment in
-
Preservation of Residual Kidney Function and Urine Volume in Patients on Dialysis.Clin J Am Soc Nephrol. 2017 Mar 7;12(3):377-379. doi: 10.2215/CJN.00330117. Epub 2017 Feb 22. Clin J Am Soc Nephrol. 2017. PMID: 28228463 Free PMC article. No abstract available.
References
-
- Maiorca R, Brunori G, Zubani R, Cancarini GC, Manili L, Camerini C, Movilli E, Pola A, d’Avolio G, Gelatti U: Predictive value of dialysis adequacy and nutritional indices for mortality and morbidity in CAPD and HD patients. A longitudinal study. Nephrol Dial Transplant 10: 2295–2305, 1995 - PubMed
-
- Canada-USA (CANUSA) Peritoneal Dialysis Study Group : Adequacy of dialysis and nutrition in continuous peritoneal dialysis: Association with clinical outcomes. Canada-USA (CANUSA) Peritoneal Dialysis Study Group. J Am Soc Nephrol 7: 198–207, 1996 - PubMed
-
- Diaz-Buxo JA, Lowrie EG, Lew NL, Zhang SM, Zhu X, Lazarus JM: Associates of mortality among peritoneal dialysis patients with special reference to peritoneal transport rates and solute clearance. Am J Kidney Dis 33: 523–534, 1999 - PubMed
-
- Szeto CC, Wong TY, Leung CB, Wang AY, Law MC, Lui SF, Li PK: Importance of dialysis adequacy in mortality and morbidity of chinese CAPD patients. Kidney Int 58: 400–407, 2000 - PubMed
-
- Bargman JM, Thorpe KE, Churchill DN; CANUSA Peritoneal Dialysis Study Group : Relative contribution of residual renal function and peritoneal clearance to adequacy of dialysis: A reanalysis of the CANUSA study. J Am Soc Nephrol 12: 2158–2162, 2001 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
