

Gender differences in clinical presentation and 1-year outcomes in atrial fibrillation
- PMID: 28228467
- PMCID: PMC5529986
- DOI: 10.1136/heartjnl-2016-310406
Gender differences in clinical presentation and 1-year outcomes in atrial fibrillation
Abstract
Objectives: Our objective was to examine gender differences in clinical presentation, management and prognosis of atrial fibrillation (AF) in a contemporary cohort.
Methods: In 6412 patients, 39.7% women, of the PREvention oF thromboembolic events - European Registry in Atrial Fibrillation, we examined gender differences in symptoms, risk factors, therapies and 1-year incidence of adverse outcomes.
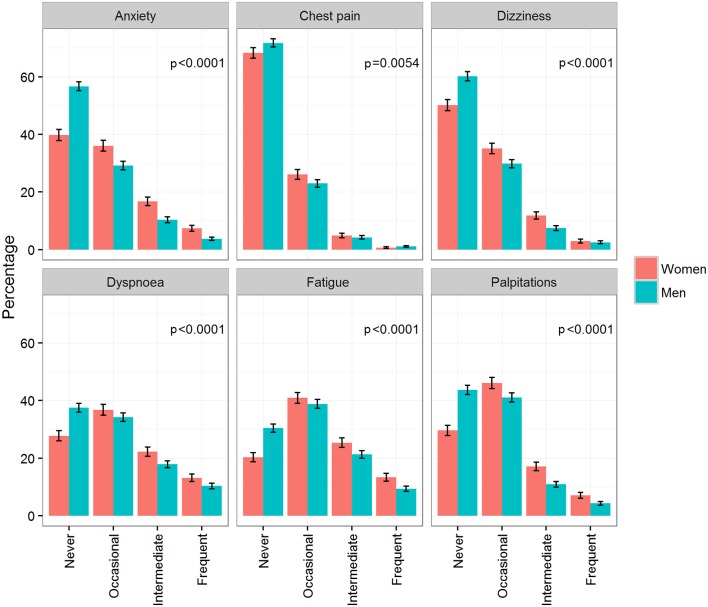
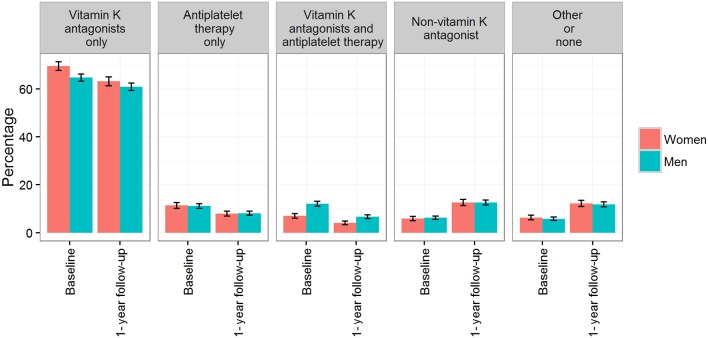
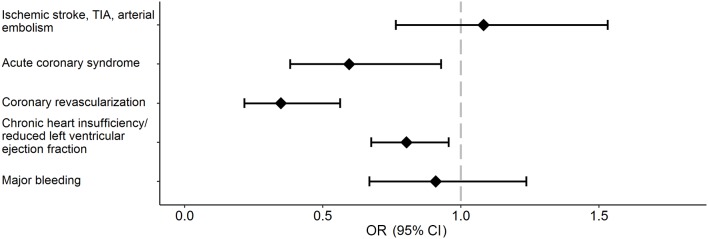
Results: Men with AF were on average younger than women (mean±SD: 70.1±10.7 vs 74.1±9.7 years, p<0.0001). Women more frequently had at least one AF-related symptom at least occasionally compared with men (95.4% in women, 89.8% in men, p<0.0001). Prescription of oral anticoagulation was similar, with an increase of non-vitamin K antagonist oral anticoagulants from 5.9% to 12.6% in women and from 6.2% to 12.6% in men, p<0.0001 for both.Men were more frequently treated with electrical cardioversion and ablation (20.6% and 6.3%, respectively) than women (14.9% and 3.3%, respectively), p<0.0001. Women had 65% (OR: 0.35; 95% CI (0.22 to 0.56)) lower age-adjusted and country-adjusted odds of coronary revascularisation, 40% (OR: 0.60; (0.38 to 0.93)) lower odds of acute coronary syndrome and 20% (OR: 0.80; (0.68 to 0.96)) lower odds of heart failure at 1 year. There were no statistically significant gender differences in 1-year stroke/transient ischaemic attack/arterial thromboembolism and major bleeding events.
Conclusion: In a 'real-world' European AF registry, women were more symptomatic but less likely to receive invasive rhythm control therapy such as electrical cardioversion or ablation. Further study is needed to confirm that these differences do not disadvantage women with AF.
Keywords: Atrial fibrillation; European registry; gender differences.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: The PREFER in AF study sponsor via a contract research organisation (SSS International Clinical Research GmbH, Munich, Germany) was Daiichi Sankyo Europe GmbH, Munich. The study has an independent scientific steering committee. RDC reports that his institution received research grant support from Boehringer-Ingelheim, Bayer, Bristol-Myers Squibb/Pfizer and Roche and honoraria for lectures and/or consulting from Boehringer-Ingelheim, Bayer and Bristol-Myers Squibb/Pfizer, Daiichi Sankyo, Lilly, AstraZeneca, Merck and Novartis. PK receives further research support from the European Union (grant agreement number 633193 (CATCH ME)), British Heart Foundation (FS/13/43/30324), Medical Research Council (UK), Leducq Foundation, German Centre for Heart Research and several drug and device companies active in atrial fibrillation and has received honoraria from several such companies. He is listed as an inventor on two pending patents (WO 2015140571 and WO 2016012783) filed by the University of Birmingham. DK reports grants from Menarini outside the submitted work but during the conduct of the study and professional development support from Daiichi Sankyo.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials