

Primary neuroendocrine carcinoma of the breast: report of 2 cases and literature review
- PMID: 28228868
- PMCID: PMC5310536
- DOI: 10.1016/j.radcr.2016.12.001
Primary neuroendocrine carcinoma of the breast: report of 2 cases and literature review
Abstract
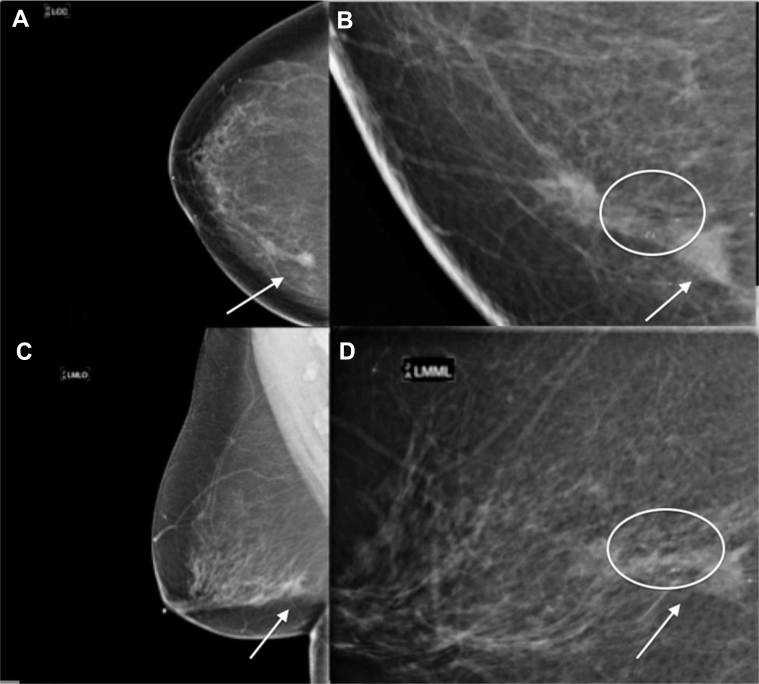
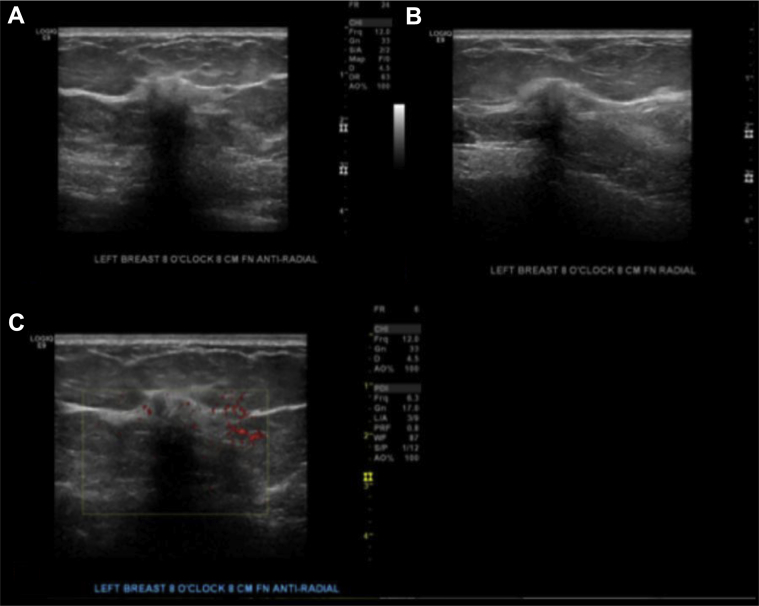
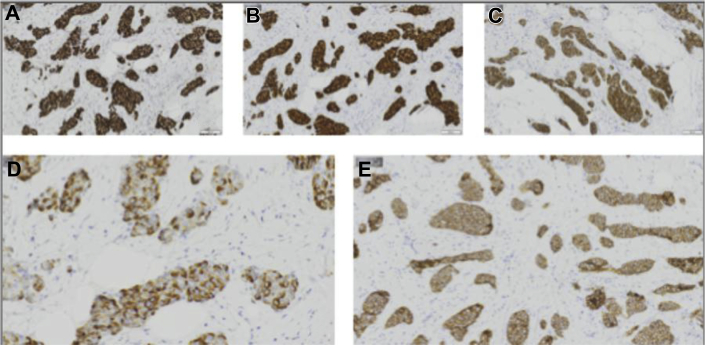
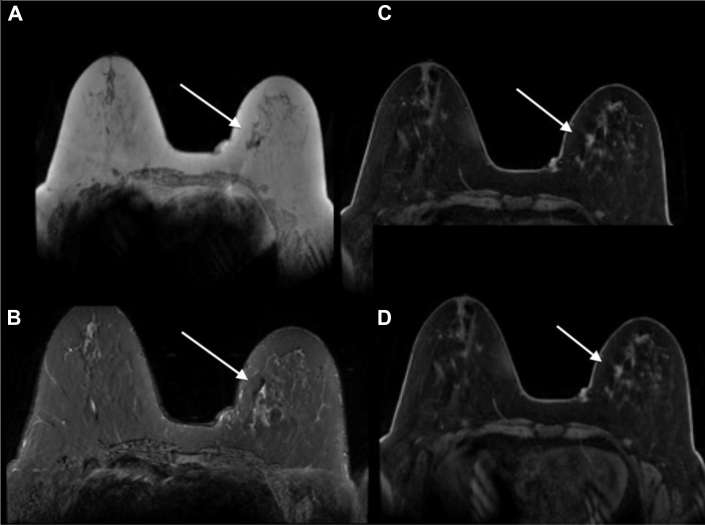
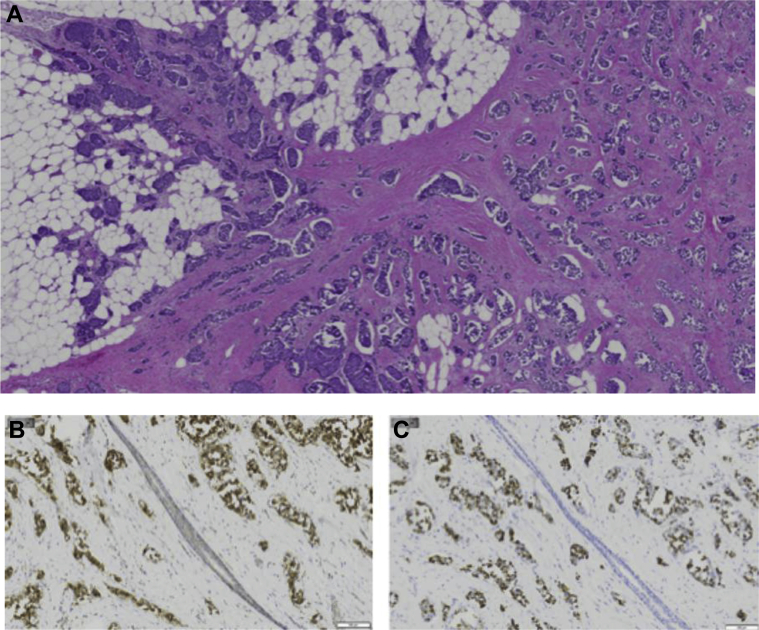
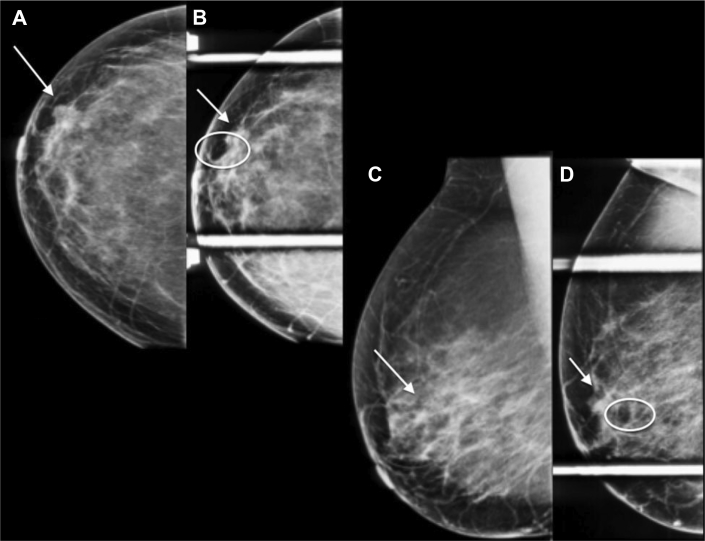
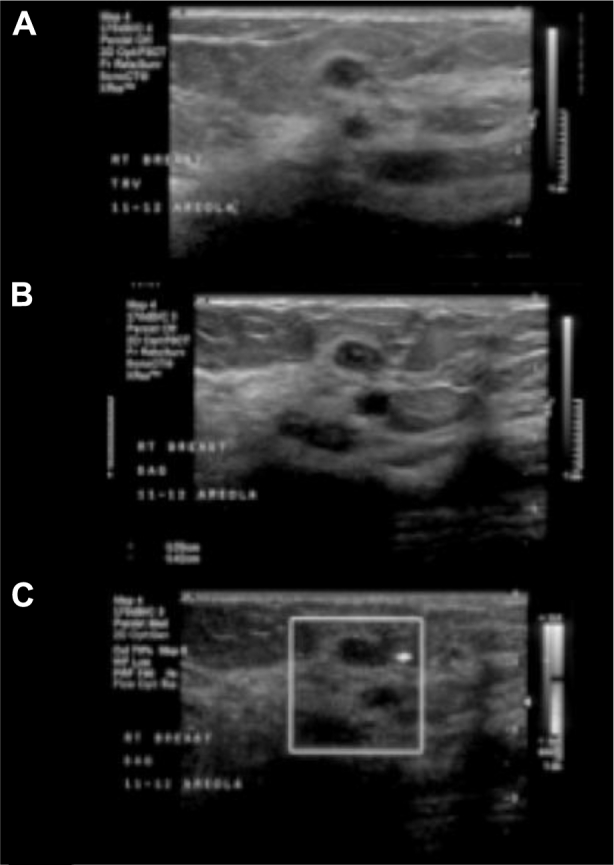
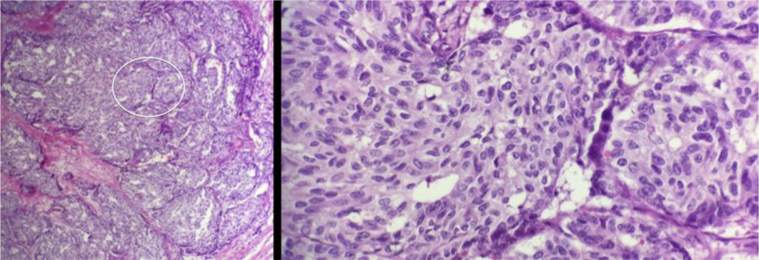
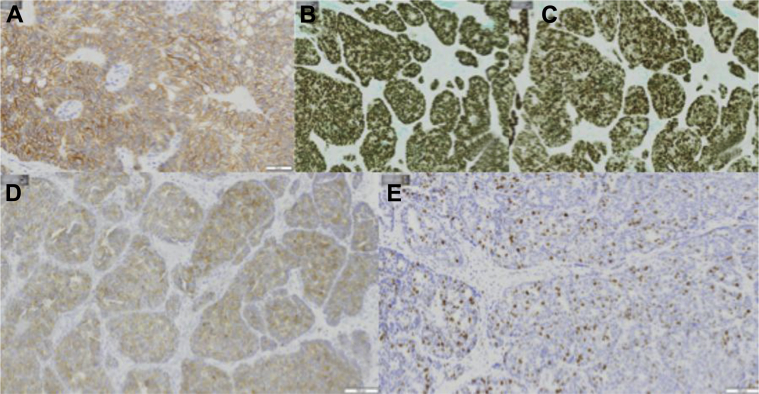
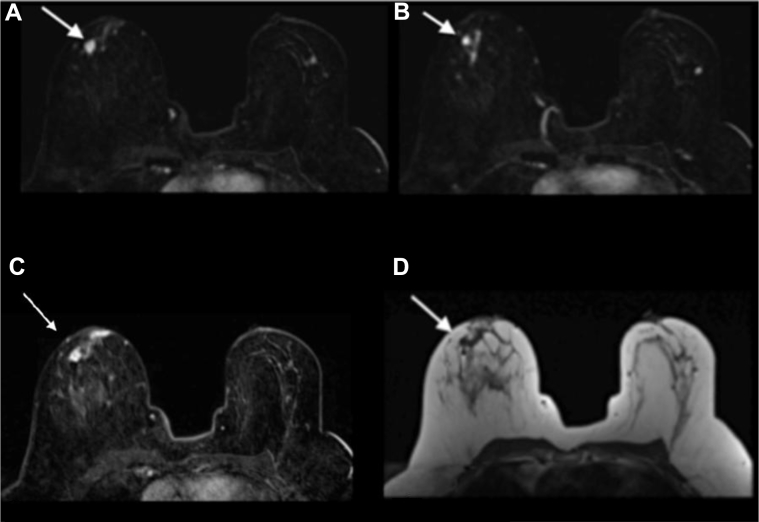
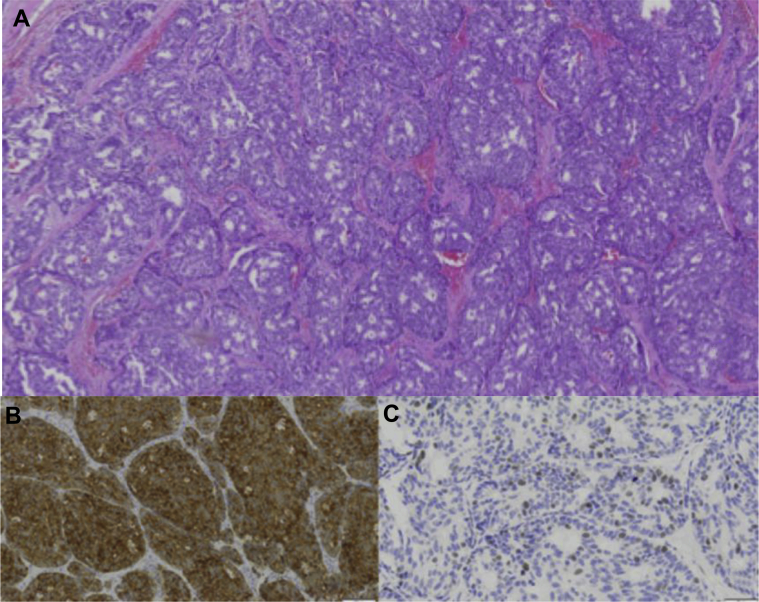
Neuroendocrine tumors of the breast are very rare accounting for less than 0.1% of all breast cancers and less than 1% of all neuroendocrine tumors. Focal neuroendocrine differentiation can be found in different histologic types of breast carcinoma including in situ and invasive ductal or invasive lobular. However, primary neuroendocrine carcinoma of the breast requires the expression of neuroendocrine markers in more than 50% of the cell population, the presence of ductal carcinoma in situ, and the absence of clinical evidence of concurrent primary neuroendocrine carcinoma of any other organ. Reports discussing the imaging characteristics of this rare carcinoma in different breast imaging modalities are scarce. We present 2 cases of primary neuroendocrine carcinoma of the breast for which mammography, ultrasound, and magnetic resonance imaging findings and pathology findings are described. A review of the medical literature on this particular topic was performed, and the results are presented.
Keywords: Breast; Carcinoma; MRI; Mammogram; Neuroendocrine; Ultrasound.
Figures

References
-
- Ogawa H., Nishio A., Satake H., Naganawa S., Imai T., Sawaki M. Neuroendocrine tumor in the breast. Radiat Med. 2008;26(1):28–32. - PubMed
-
- Ajisaka H., Maeda K., Miwa A. Breast cancer with endocrine differentiation: report of two cases showing different histologic patterns. Surg Today. 2003;22:909–912. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
