

Imaging of Cholangiocarcinoma
- PMID: 28229074
- PMCID: PMC5290452
- DOI: 10.1159/000453009
Imaging of Cholangiocarcinoma
Abstract
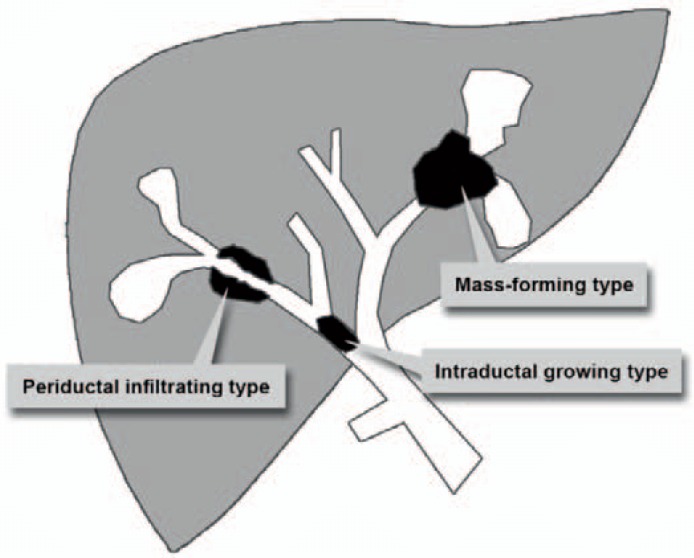
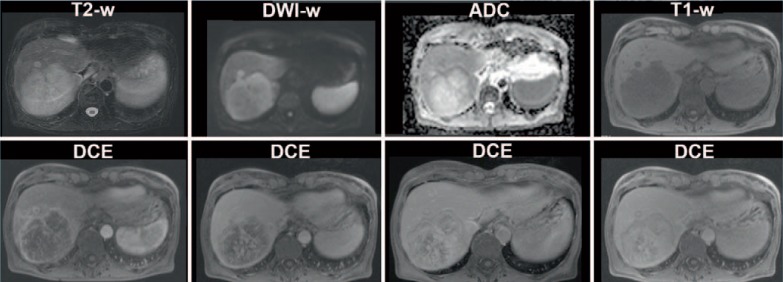
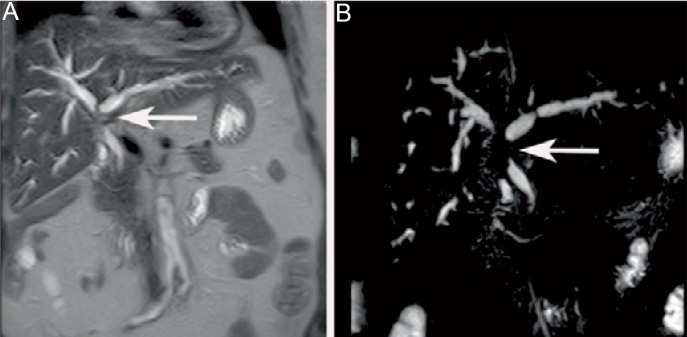
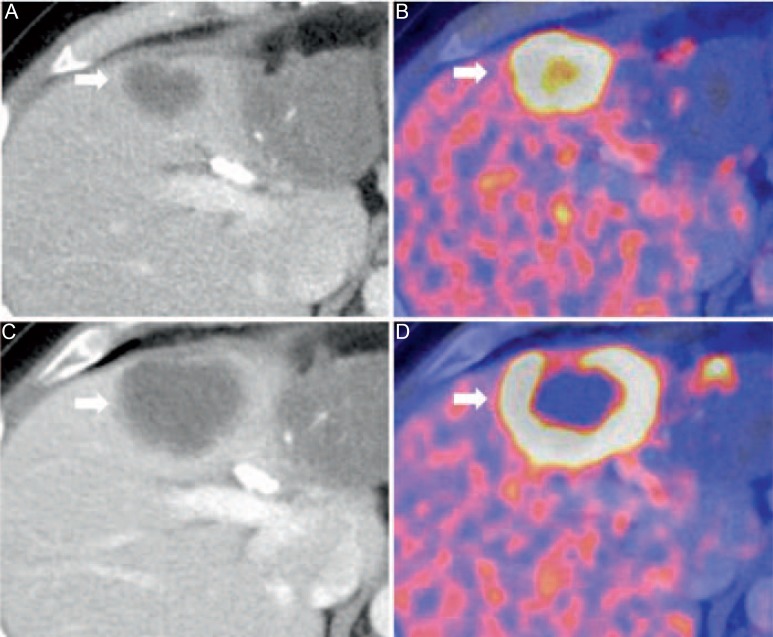
Cholangiocarcinoma (CC) is the second most common primary hepatobiliary tumour, and it is increasing in incidence. Imaging characteristics, behaviour, and therapeutic strategies in CC differ significantly, depending on the morphology and location of the tumour. In cross-sectional imaging, CCs can be classified according to the growth pattern (mass-forming, periductal infiltrating, intraductal) and the location (intrahepatic, perihilar, extrahepatic/distal). The prognosis of CC is unfavourable and surgical resection is the only curative treatment option; thus, early diagnosis (also in recurrent disease) and accurate staging including the evaluation of lymph node involvement and vascular infiltration is crucial. However, the diagnostic evaluation of CC is challenging due to the heterogeneous nature of the tumour. Diagnostic modalities used in the imaging of CC include transabdominal ultrasound, endosonography, computed tomography, magnetic resonance imaging with cholangiopancreatography, and hybrid imaging such as positron emission tomography/computed tomography. In this review, the potential of cross-sectional imaging modalities in primary staging, treatment monitoring, and detection of recurrent disease will be discussed.
Keywords: Cholangiocarcinoma; Computed tomography; Cross-sectional imaging; Magnetic resonance imaging; Positron emission tomography.
Figures


References
-
- Patel T, Singh P. Cholangiocarcinoma: emerging approaches to a challenging cancer. Curr Opin Gastroenterol. 2007;23:317–323. - PubMed
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24:115–125. - PubMed
-
- Khan SA, Thomas HC, Davidson BR, Taylor-Robinson SD. Cholangiocarcinoma. Lancet. 2005;366:1303–1314. - PubMed
-
- Shaib YH, Davila JA, McGlynn K, El-Serag HB. Rising incidence of intrahepatic cholangiocarcinoma in the United States: a true increase? J Hepatol. 2004;40:472–477. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
