

Are cardiovascular risk factors also associated with the incidence of atrial fibrillation? A systematic review and field synopsis of 23 factors in 32 population-based cohorts of 20 million participants
- PMID: 28229164
- PMCID: PMC5442605
- DOI: 10.1160/TH16-11-0825
Are cardiovascular risk factors also associated with the incidence of atrial fibrillation? A systematic review and field synopsis of 23 factors in 32 population-based cohorts of 20 million participants
Abstract
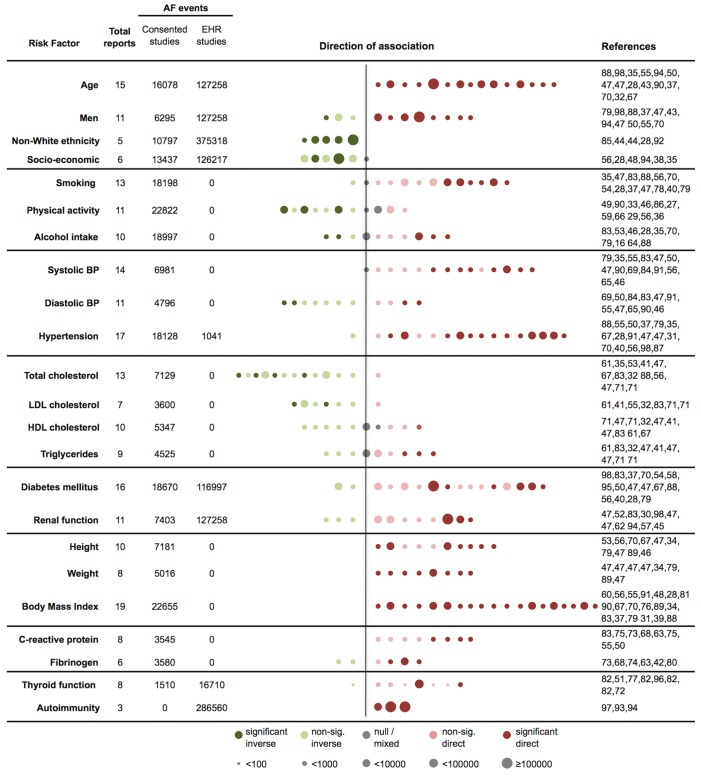
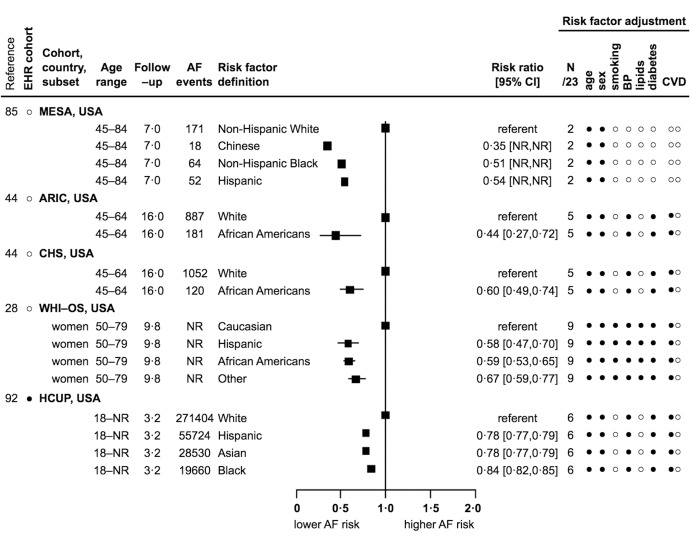
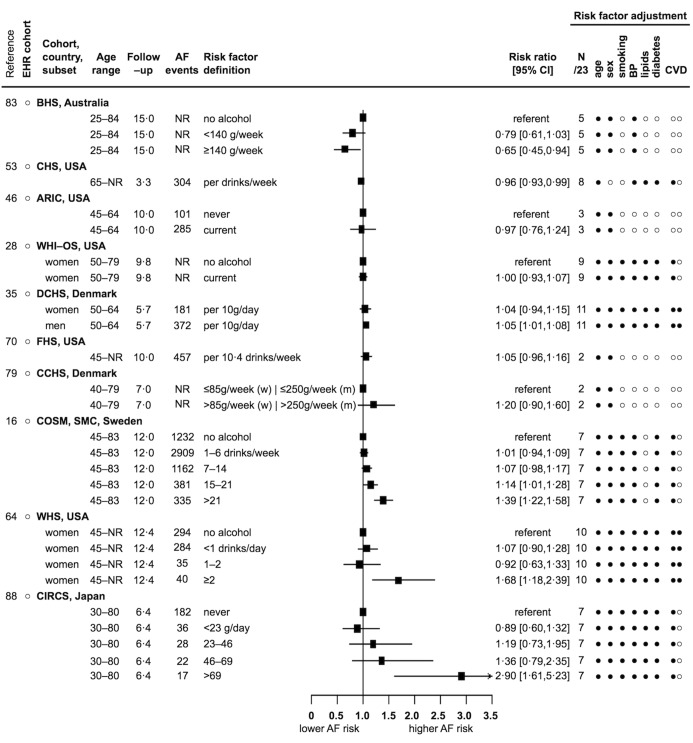
Established primary prevention strategies of cardiovascular diseases are based on understanding of risk factors, but whether the same risk factors are associated with atrial fibrillation (AF) remains unclear. We conducted a systematic review and field synopsis of the associations of 23 cardiovascular risk factors and incident AF, which included 84 reports based on 28 consented and four electronic health record cohorts of 20,420,175 participants and 576,602 AF events. We identified 3-19 reports per risk factor and heterogeneity in AF definition, quality of reporting, and adjustment. We extracted relative risks (RR) and 95 % confidence intervals [CI] and visualised the number of reports with inverse (RR [CI]<1.00), or direct (RR [CI]>1.00) associations. For hypertension (13/17 reports) and obesity (19/19 reports), there were direct associations with incident AF, as there are for coronary heart disease (CHD). There were inverse associations for non-White ethnicity (5/5 reports, with RR from 0.35 to 0.84 [0.82-0.85]), total cholesterol (4/13 reports from 0.76 [0.59-0.98] to 0.94 [0.90-0.97]; 8/13 reports with non-significant inverse associations), and diastolic blood pressure (2/11 reports from 0.87 [0.78-0.96] to 0.92 [0.85-0.99]; 5/11 reports with non-significant inverse associations), and direct associations for taller height (7/10 reports from 1.03 [1.02-1.05] to 1.92 [1.38-2.67]), which are in the opposite direction of known associations with CHD. A systematic evaluation of the available evidence suggests similarities as well as important differences in the risk factors for incidence of AF as compared with other cardiovascular diseases, which has implications for the primary prevention strategies for atrial fibrillation.
Keywords: Atrial fibrillation; cardiovascular disease; clinical guidelines; primary prevention; risk factors.
Conflict of interest statement
None declared.
Figures



References
-
- Marini C, et al. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke 2005; 36: 1115–1119. - PubMed
-
- Benjamin EJ, et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation 1998; 98: 946–952. - PubMed
-
- Blomstrom Lundqvist C, et al. What are the costs of atrial fibrillation? Europace 2011; 13 (Suppl 2): ii9–12. - PubMed
-
- Miyasaka Y, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to. 2000, and implications on the projections for future prevalence. Circulation 2006; 114: 119–125. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical