

Prevalence and clinical impact of iron deficiency and anaemia among outpatients with chronic heart failure: The PrEP Registry
- PMID: 28229219
- PMCID: PMC5442200
- DOI: 10.1007/s00392-016-1073-y
Prevalence and clinical impact of iron deficiency and anaemia among outpatients with chronic heart failure: The PrEP Registry
Abstract
Background: Iron deficiency (ID) and anaemia are common in heart failure (HF). The prospective, observational PReP registry (Prävalenz des Eisenmangels bei Patienten mit Herzinsuffizienz) studied prevalence and clinical impact of ID and anaemia in HF outpatients attending cardiology practices in Germany.
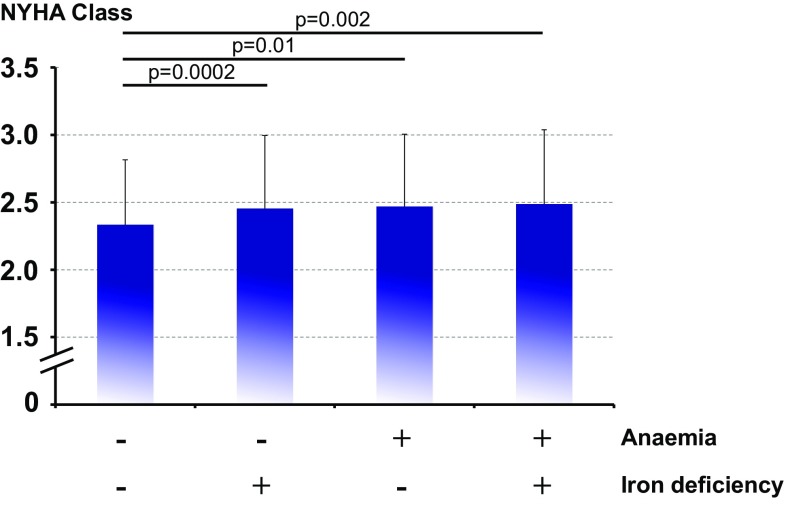
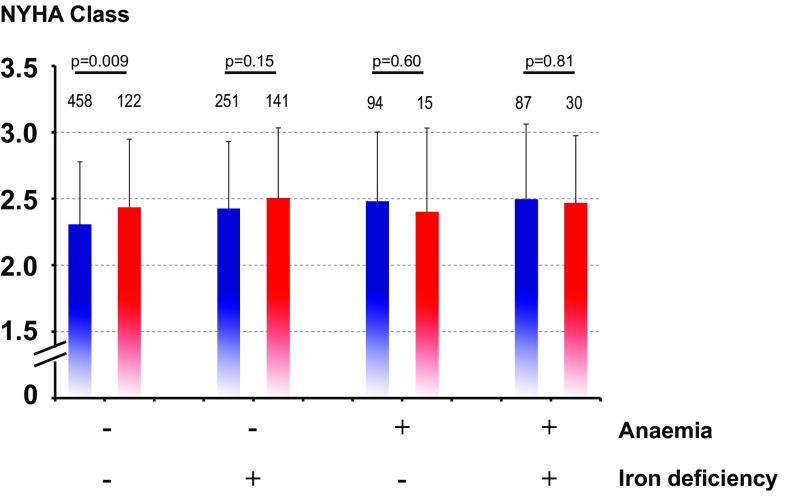
Methods and results: A total of 42 practices enrolled consecutive patients with chronic HF [left ventricular ejection fraction (LVEF) ≤45%]. ID was defined as serum ferritin <100 µg/l, or serum ferritin ≥100 µg/l/<300 µg/l plus transferrin saturation <20%, and anaemia as haemoglobin <13 g/dl (12 g/dl) in men (women). Exercise capacity was assessed using spiroergometry (69.4%) or 6-min walk test (30.4%). Amongst 1198 PReP-participants [69.0 ± 10.6 years, 25.3% female, New York Heart Association (NYHA) class 2.4 ± 0.5, LVEF 35.3 ± 7.2%], ID was found in 42.5% (previously unknown in all), and anaemia in 18.9% (previously known in 4.8%). ID was associated with female gender, lower body weight and haemoglobin, higher NYHA class and natriuretic peptide (NP) levels (all p < 0.05). ID was also more common in anaemic than non-anaemic patients (p < 0.0001), and 9.8% of PrEP-participants had both, ID and anaemia. On spiroergometry, ID independently predicted maximum exercise capacity even after multivariable adjustment, including anaemia (p = 0.0004). In all PrEP-participants, ID predicted reduced physical performance (adjusted for age, gender, anaemia, serum creatinine, C-reactive protein, LVEF, and NP level).
Conclusions: Despite high prevalence, ID was previously unknown in all PrEP-participants, and anaemia was often unappreciated. Given the clinical relevance, treatability, and independent association with reduced physical performance, ID should be considered more in real-world ambulatory healthcare settings and ID-screening be advocated to cardiologists in such populations.
Keywords: Anaemia; Exercise capacity; Heart failure; Iron deficiency; Prevalence.
Conflict of interest statement
Funding
This work was supported by Vifor Pharma.
Conflict of interest
SvH has received consulting honoraria from Vifor Pharma and lecture fees from Amgen. C.E. Angermann acknowledges grant and other support, speaker honoraria, and consultancy fees from Vifor Pharma. All other authors have no conflicts of interest relevant to this manuscript to disclose.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, on behalt of the Authors/Task Force Members and Document Reviewers ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (ESC) developed with the special contribution of the heart failure association (HFA) of the ESC. Eur J Heart Fail. 2016;18:891–975. doi: 10.1002/ejhf.592. - DOI - PubMed
-
- Beard JL. Iron biology in immune function, muscle metabolism and neuronal functioning. J Nutr 2001;131(Suppl 2):568S–579S - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
