

4D dose simulation in volumetric arc therapy: Accuracy and affecting parameters
- PMID: 28231337
- PMCID: PMC5322962
- DOI: 10.1371/journal.pone.0172810
4D dose simulation in volumetric arc therapy: Accuracy and affecting parameters
Abstract
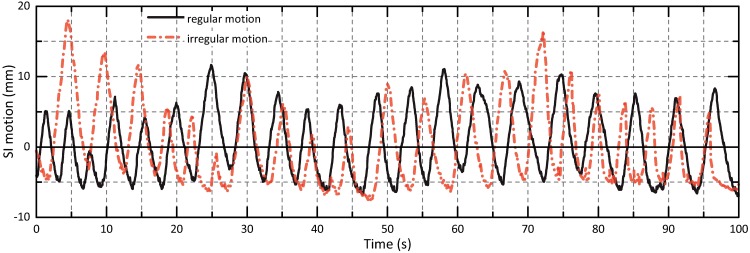
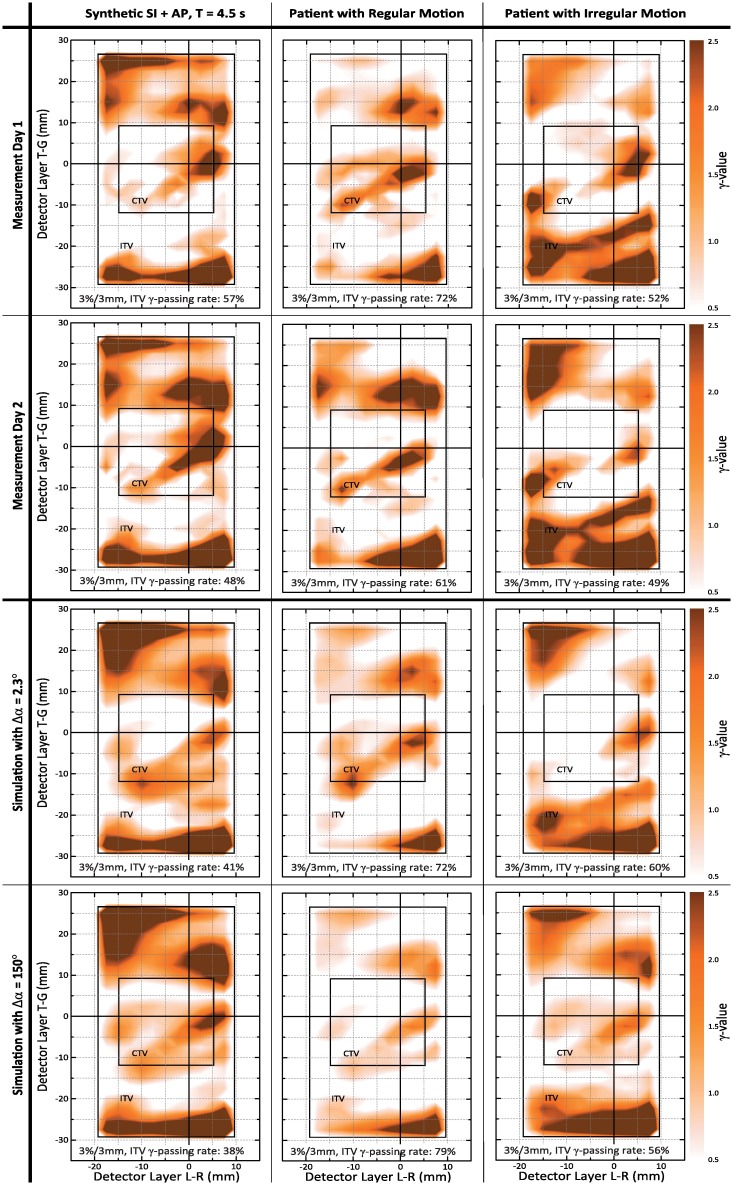
Radiotherapy of lung and liver lesions has changed from normofractioned 3D-CRT to stereotactic treatment in a single or few fractions, often employing volumetric arc therapy (VMAT)-based techniques. Potential unintended interference of respiratory target motion and dynamically changing beam parameters during VMAT dose delivery motivates establishing 4D quality assurance (4D QA) procedures to assess appropriateness of generated VMAT treatment plans when taking into account patient-specific motion characteristics. Current approaches are motion phantom-based 4D QA and image-based 4D VMAT dose simulation. Whereas phantom-based 4D QA is usually restricted to a small number of measurements, the computational approaches allow simulating many motion scenarios. However, 4D VMAT dose simulation depends on various input parameters, influencing estimated doses along with mitigating simulation reliability. Thus, aiming at routine use of simulation-based 4D VMAT QA, the impact of such parameters as well as the overall accuracy of the 4D VMAT dose simulation has to be studied in detail-which is the topic of the present work. In detail, we introduce the principles of 4D VMAT dose simulation, identify influencing parameters and assess their impact on 4D dose simulation accuracy by comparison of simulated motion-affected dose distributions to corresponding dosimetric motion phantom measurements. Exploiting an ITV-based treatment planning approach, VMAT treatment plans were generated for a motion phantom and different motion scenarios (sinusoidal motion of different period/direction; regular/irregular motion). 4D VMAT dose simulation results and dose measurements were compared by local 3% / 3 mm γ-evaluation, with the measured dose distributions serving as ground truth. Overall γ-passing rates of simulations and dynamic measurements ranged from 97% to 100% (mean across all motion scenarios: 98% ± 1%); corresponding values for comparison of different day repeat measurements were between 98% and 100%. Parameters of major influence on 4D VMAT dose simulation accuracy were the degree of temporal discretization of the dose delivery process (the higher, the better) and correct alignment of the assumed breathing phases at the beginning of the dose measurements and simulations. Given the high γ-passing rates between simulated motion-affected doses and dynamic measurements, we consider the simulations to provide a reliable basis for assessment of VMAT motion effects that-in the sense of 4D QA of VMAT treatment plans-allows to verify target coverage in hypofractioned VMAT-based radiotherapy of moving targets. Remaining differences between measurements and simulations motivate, however, further detailed studies.
Conflict of interest statement
Figures



Similar articles
-
4D VMAT planning and verification technique for dynamic tracking using a direct aperture deformation (DAD) method.J Appl Clin Med Phys. 2017 Mar;18(2):50-61. doi: 10.1002/acm2.12053. Epub 2017 Mar 6. J Appl Clin Med Phys. 2017. PMID: 28300367 Free PMC article.
-
Motion as a perturbation: measurement-guided dose estimates to moving patient voxels during modulated arc deliveries.Med Phys. 2013 Feb;40(2):021708. doi: 10.1118/1.4773887. Med Phys. 2013. PMID: 23387731
-
Simulation of dosimetry impact of 4DCT uncertainty in 4D dose calculation for lung SBRT.Radiat Oncol. 2019 Jan 8;14(1):1. doi: 10.1186/s13014-018-1191-y. Radiat Oncol. 2019. PMID: 30621744 Free PMC article.
-
Influence of the jaw tracking technique on the dose calculation accuracy of small field VMAT plans.J Appl Clin Med Phys. 2017 Jan;18(1):186-195. doi: 10.1002/acm2.12029. Epub 2017 Jan 3. J Appl Clin Med Phys. 2017. PMID: 28291941 Free PMC article. Review.
-
Applications of machine and deep learning to patient-specific IMRT/VMAT quality assurance.J Appl Clin Med Phys. 2021 Sep;22(9):20-36. doi: 10.1002/acm2.13375. Epub 2021 Aug 3. J Appl Clin Med Phys. 2021. PMID: 34343412 Free PMC article. Review.
Cited by
-
Adoption of respiratory motion management in radiation therapy.Phys Imaging Radiat Oncol. 2022 Sep 13;24:21-29. doi: 10.1016/j.phro.2022.09.003. eCollection 2022 Oct. Phys Imaging Radiat Oncol. 2022. PMID: 36148153 Free PMC article.
-
Technological quality requirements for stereotactic radiotherapy : Expert review group consensus from the DGMP Working Group for Physics and Technology in Stereotactic Radiotherapy.Strahlenther Onkol. 2020 May;196(5):421-443. doi: 10.1007/s00066-020-01583-2. Epub 2020 Mar 24. Strahlenther Onkol. 2020. PMID: 32211939 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
