

Early evaluation of sunitinib for the treatment of advanced gastroenteropancreatic neuroendocrine neoplasms via CT imaging: RECIST 1.1 or Choi Criteria?
- PMID: 28231773
- PMCID: PMC5324282
- DOI: 10.1186/s12885-017-3150-7
Early evaluation of sunitinib for the treatment of advanced gastroenteropancreatic neuroendocrine neoplasms via CT imaging: RECIST 1.1 or Choi Criteria?
Abstract
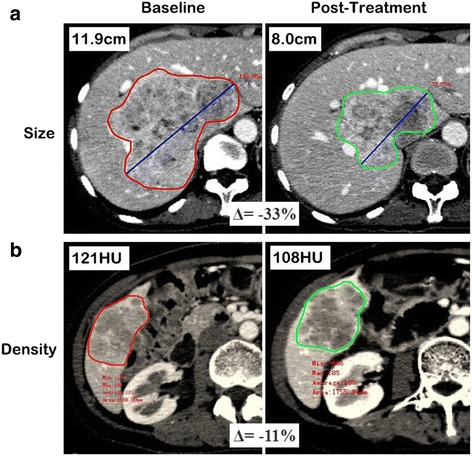
Background: The aim of this study was to assess and compare the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1) and the Choi criteria in evaluating the early response of advanced gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs) treated with sunitinib.
Methods: Eighteen patients with pathologically proven advanced GEP-NENs treated with sunitinib were enrolled in the study. Pre- and post-treatment CT scans (plain, biphasic enhanced CT scan) were performed on all patients. Changes in the target tumor size and density from pre-treatment to 1.4-3.1 months after treatment were measured and recorded for each patient. Tumor responses were identified using RECIST 1.1 and Choi criteria. The time to tumor progression (TTP) for each patient was measured and compared between groups using the Kaplan-Meier method.
Results: Among the 18 patients, 4 (22%) exhibited a partial response (PR), 9 (50%) exhibited stable disease (SD), and 5 (28%) experienced progressive disease (PD), using RECIST 1.1. However, based on the Choi criteria, 8 (44%) patients exhibited a PR, 4 (22%) exhibited SD, and 6 (33%) experienced PD. According to RECIST 1.1, the median TTP of PR, SD and PD group were 16.6, 10.8 and 2.3 months, respectively. The TTP of the PR group was significantly longer than that of the PD group (P = 0.007) but insignificant when compared to the SD group (P = 0.131). According to Choi criteria, the median TTP of PR, SD and PD group were not reached, 10.8 and 2.3 months, respectively. The TTP of the PR group was significantly longer than that of the SD (P = 0.026) and PD groups (P < 0.001).
Conclusion: The Choi criteria appear to be more sensitive and more precise than RECIST 1.1 in assessing the early response of advanced GEP-NENs treated with sunitinib.
Keywords: Computed tomography; Gastroenteropancreatic neuroendocrine neoplasms; Sunitinib; Time to tumor progression.
Figures




References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
