

SOFA and mortality endpoints in randomized controlled trials: a systematic review and meta-regression analysis
- PMID: 28231816
- PMCID: PMC5324238
- DOI: 10.1186/s13054-017-1609-1
SOFA and mortality endpoints in randomized controlled trials: a systematic review and meta-regression analysis
Abstract
Background: The sequential organ failure assessment score (SOFA) is increasingly used as an endpoint in intensive care randomized controlled trials (RCTs). Although serially measured SOFA is independently associated with mortality in observational cohorts, the association between treatment effects on SOFA vs. effects on mortality has not yet been quantified in RCTs. The aim of this study was to quantify the relationship between SOFA and mortality in RCTs and to identify which SOFA derivative best reflects between-group mortality differences.
Methods: The review protocol was prospectively registered (Prospero CRD42016034014). We performed a literature search (up to May 1, 2016) for RCTs reporting both SOFA and mortality, and analyzed between-group differences in these outcomes. Treatment effects on SOFA and mortality were calculated as the between-group SOFA standardized difference and log odds ratio (OR), respectively. We used random-effects meta-regression to (1) quantify the linear relationship between RCT treatment effects on mortality (logOR) and SOFA (i.e. responsiveness) and (2) quantify residual heterogeneity (i.e. consistency, expressed as I 2).
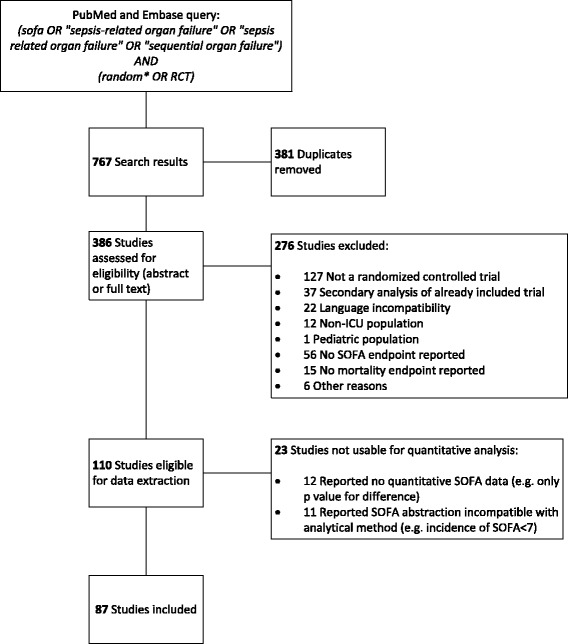
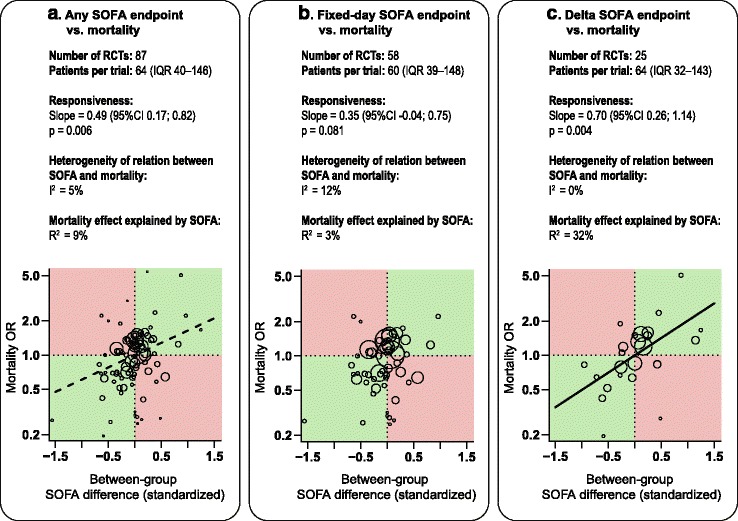
Results: Of 110 eligible RCTs, 87 qualified for analysis. Using all RCTs, SOFA was significantly associated with mortality (slope = 0.49 (95% CI 0.17; 0.82), p = 0.006, I 2 = 5%); the overall mortality effect explained by SOFA score (R 2) was 9%. Fifty-eight RCTs used Fixed-day SOFA as an endpoint (i.e. the score on a fixed day after randomization), 25 studies used Delta SOFA as an endpoint (i.e. the trajectory from baseline score) and 15 studies used other SOFA derivatives as an endpoint. Fixed-day SOFA was not significantly associated with mortality (slope = 0.35 (95% CI -0.04; 0.75), p = 0.08, I 2 = 12%) and explained 3% of the overall mortality effect (R 2). Delta SOFA was significantly associated with mortality (slope = 0.70 (95% CI 0.26; 1.14), p = 0.004, I 2 = 0%) and explained 32% of the overall mortality effect (R 2).
Conclusions: Treatment effects on Delta SOFA appear to be reliably and consistently associated with mortality in RCTs. Fixed-day SOFA was the most frequently reported outcome among the reviewed RCTs, but was not significantly associated with mortality. Based on this study, we recommend using Delta SOFA rather than Fixed-day SOFA as an endpoint in future RCTs.
Keywords: Critical care trials; Multiple organ failure; Sepsis; Surrogate endpoints.
Figures
References
-
- Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–10. doi: 10.1007/BF01709751. - DOI - PubMed
-
- Moreno R, Vincent JL, Matos R, Mendonça A, Cantraine F, Thijs L, et al. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Working Group on Sepsis related Problems of the ESICM. Intensive Care Med. 1999;25:686–96. doi: 10.1007/s001340050931. - DOI - PubMed
-
- Rubenfeld GD. Surrogate Measures of Patient-centered Outcomes in Critical Care. In: Angus DC, Carlet J, editors. Surviv. Intensive Care. Berlin: Springer; 2003. pp. 169–80.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
