

Knee tissue lesions and prediction of incident knee osteoarthritis over 7 years in a cohort of persons at higher risk
- PMID: 28232012
- PMCID: PMC5466844
- DOI: 10.1016/j.joca.2017.02.788
Knee tissue lesions and prediction of incident knee osteoarthritis over 7 years in a cohort of persons at higher risk
Abstract
Objective: Among high risk individuals, whether knee lesions in tissues involved in osteoarthritis (OA) can improve prediction of knee OA is unclear. We hypothesized that models predicting (1) incident osteophytes and (2) incident osteophytes and joint space narrowing can be improved by including symptoms or function, and further improved by lesion status.
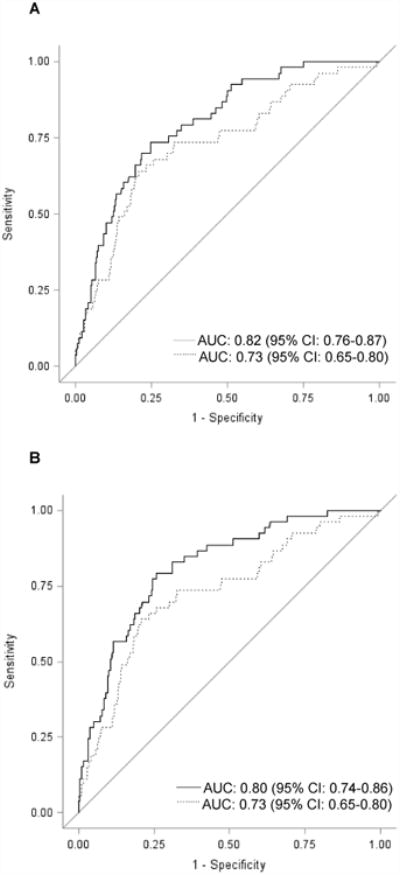
Design: In Osteoarthritis Initiative (OAI) participants with normal knee X-rays, we assessed cartilage damage, bone marrow lesions (BMLs), and menisci. Cox proportional hazards models were used to develop risk prediction models for risk of each outcome. Nested models (increasingly larger baseline covariable sets) were compared using likelihood ratio tests and Schwarz Bayesian Information Criterion (SBC). Model discrimination used receiver operating characteristic (ROC) curves and area under the curve (AUC).
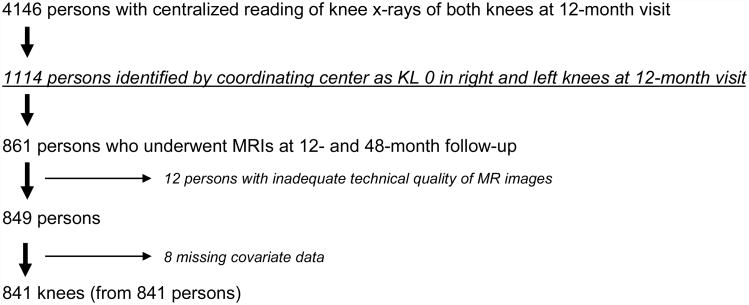
Results: In 841 participants [age 59.6, body mass index (BMI) 26.7, 55.9% women] over up to 7 years follow-up, each larger set improved prediction (+hand OA, injury, surgery, activities; +symptoms/function). Prediction was further improved by including cartilage damage both compartments, BMLs both compartments, meniscal tear, meniscal extrusion, sum of lesion types, number of subregions with cartilage damage, number of subregions with BMLs, and (concurrently) subregion number with cartilage damage, subregion number with BMLs, and meniscal tear. AUCs were ≥0.80 for both outcomes for number of subregions with cartilage damage and the combined model.
Conclusions: Among persons at higher risk for knee OA with normal X-rays, MRI tissue lesions improved prediction of mild as well as moderate disease. These findings support that disease onset is likely occurring during the "high-risk" period and encourage a reorientation of approach.
Keywords: Epidemiology; Knee osteoarthritis; Magnetic resonance imaging; Risk factors.
Copyright © 2017 Osteoarthritis Research Society International. Published by Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Clinical significance of worsening versus stable preradiographic MRI lesions in a cohort study of persons at higher risk for knee osteoarthritis.Ann Rheum Dis. 2016 Sep;75(9):1630-6. doi: 10.1136/annrheumdis-2015-208129. Epub 2015 Oct 14. Ann Rheum Dis. 2016. PMID: 26467570 Free PMC article.
-
Significance of preradiographic magnetic resonance imaging lesions in persons at increased risk of knee osteoarthritis.Arthritis Rheumatol. 2014 Jul;66(7):1811-9. doi: 10.1002/art.38611. Arthritis Rheumatol. 2014. PMID: 24974824 Free PMC article.
-
Meniscal extrusion and bone marrow lesions are associated with incident and progressive knee osteoarthritis.Osteoarthritis Cartilage. 2017 Jul;25(7):1076-1083. doi: 10.1016/j.joca.2017.02.792. Epub 2017 Feb 13. Osteoarthritis Cartilage. 2017. PMID: 28216311
-
Meniscal extrusion as booster of osteoarthritis.J Biol Regul Homeost Agents. 2017 Dec 27;31(4 Suppl 2):33-44. J Biol Regul Homeost Agents. 2017. PMID: 29202561 Review.
-
Tibial subchondral bone size and knee cartilage defects: relevance to knee osteoarthritis.Osteoarthritis Cartilage. 2007 May;15(5):479-86. doi: 10.1016/j.joca.2007.01.003. Epub 2007 Feb 8. Osteoarthritis Cartilage. 2007. PMID: 17291789 Review.
Cited by
-
Association between meniscal volume and development of knee osteoarthritis.Rheumatology (Oxford). 2021 Mar 2;60(3):1392-1399. doi: 10.1093/rheumatology/keaa522. Rheumatology (Oxford). 2021. PMID: 32974683 Free PMC article.
-
The influence of meniscal pathology in the incidence of knee osteoarthritis: a review.Skeletal Radiol. 2023 Nov;52(11):2045-2055. doi: 10.1007/s00256-022-04233-z. Epub 2022 Nov 19. Skeletal Radiol. 2023. PMID: 36402862 Review.
-
Associations amongst dynamic knee stiffness during gait, quadriceps stiffness, and the incidence of knee osteoarthritis over 24 months: a cohort study with a mediation analysis.BMC Musculoskelet Disord. 2024 Jul 3;25(1):511. doi: 10.1186/s12891-024-07618-4. BMC Musculoskelet Disord. 2024. PMID: 38961407 Free PMC article.
-
Prediction model for knee osteoarthritis using magnetic resonance-based radiomic features from the infrapatellar fat pad: data from the osteoarthritis initiative.Quant Imaging Med Surg. 2023 Jan 1;13(1):352-369. doi: 10.21037/qims-22-368. Epub 2022 Nov 17. Quant Imaging Med Surg. 2023. PMID: 36620171 Free PMC article.
-
Identification of a novel disulfidptosis-related gene signature in osteoarthritis using bioinformatics analysis and experimental validation.Sci Rep. 2025 Jan 8;15(1):1339. doi: 10.1038/s41598-025-85569-z. Sci Rep. 2025. PMID: 39779817 Free PMC article.
References
-
- Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM. A systematic review of recommendations and guidelines for the management of osteoarthritis: The chronic osteoarthritis management initiative of the U.S. bone and joint initiative. Semin Arthritis Rheum. 2014;43(6):701–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
