

Antibiotic prescribing during office hours and out-of-hours: a comparison of quality and quantity in primary care in the Netherlands
- PMID: 28232364
- PMCID: PMC5325659
- DOI: 10.3399/bjgp17X689641
Antibiotic prescribing during office hours and out-of-hours: a comparison of quality and quantity in primary care in the Netherlands
Abstract
Background: Unnecessary and non-first-choice antibiotic prescribing is a significant problem in primary care. It is often argued that irrational prescribing is higher during out-of-hours (OOH) consultations.
Aim: To obtain insight into the quantity and quality of OOH antibiotic prescribing for commonly presented infectious diseases.
Design and setting: Two two-way comparisons of 1) nationally dispensed antibiotics during office hours and OOH care, using data from the Dutch Foundation of Pharmaceutical Statistics, and 2) regional prescribing quality data from 45 primary care practices from Utrecht and its vicinity, and two large OOH services in Utrecht and Woerden.
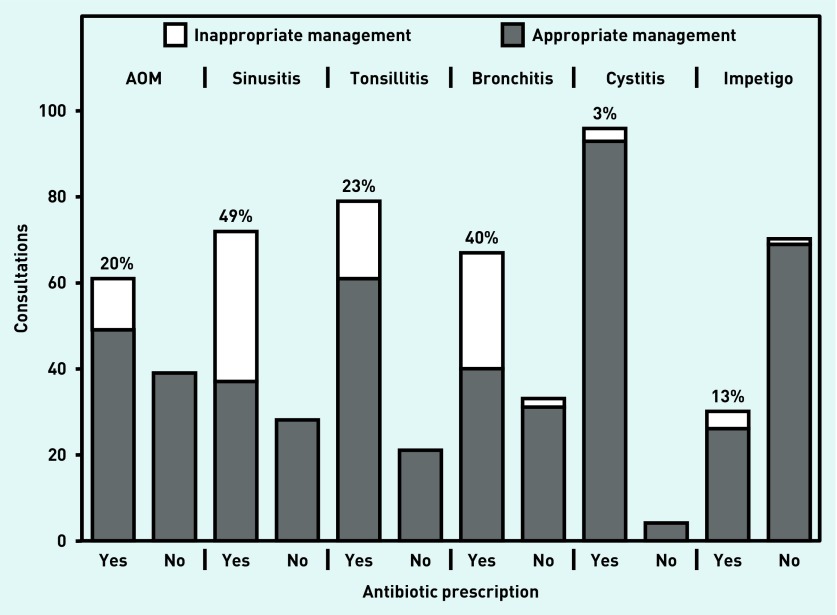
Method: From the national data, yearly dispensed antibiotics were analysed per prescriber type, with respect to time (office hours or OOH) of prescription, types of antibiotics, and patients' age group. Regional prescribing rates, choice of antibiotic, and appropriateness of prescribing were compared for otitis media, sinusitis, tonsillitis, bronchitis, cystitis, and impetigo. Appropriateness was assessed by comparing all relevant information from medical files with the guideline recommendations.
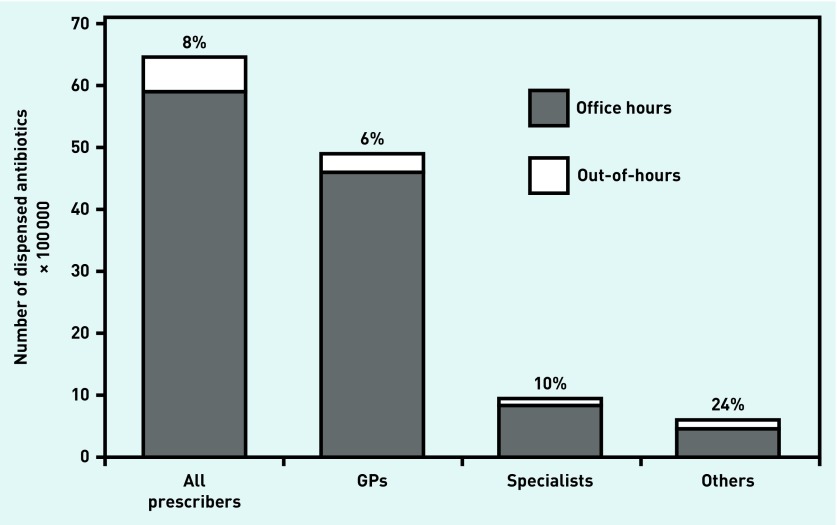
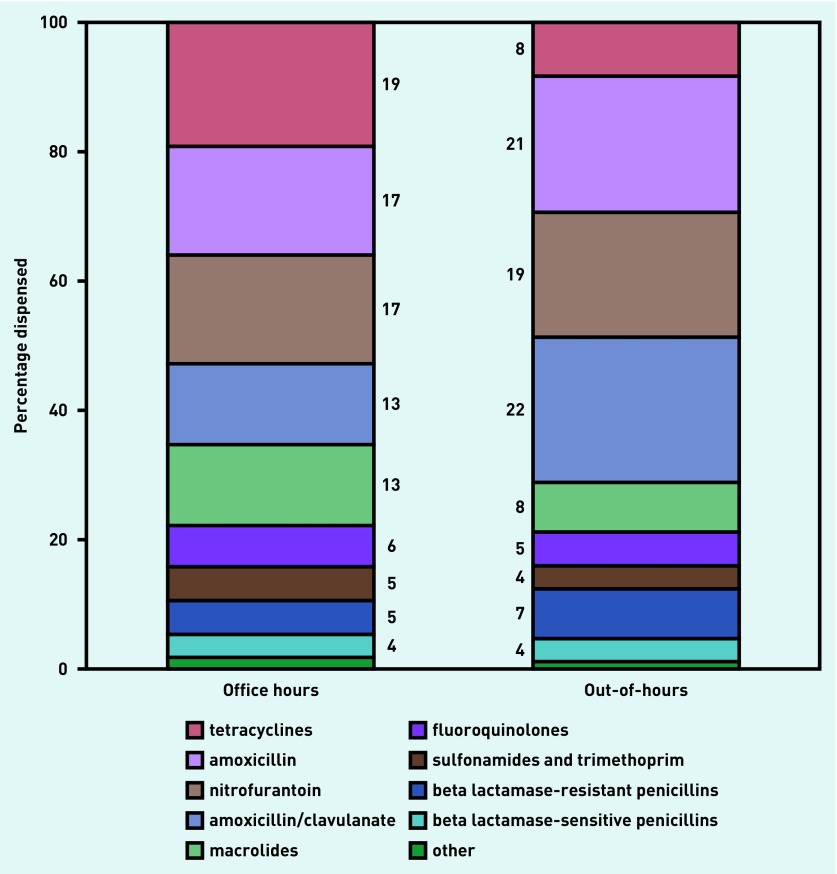
Results: Only 6% of GP-prescribed antibiotics were prescribed OOH. OOH, cystitis and acute otitis media presented most often. First-choice prescribing was comparable for the two settings, whereas prescribing rates were higher OOH, with comparatively more amoxicillin(/clavulanate). The appropriateness evaluation, however, revealed that overprescribing was comparable, or even lower than, for daily practice.
Conclusion: The suggestion that OOH antibiotic prescribing quality is worse than in daily practice does not seem founded. The higher OOH prescribing rates can be explained by a different population of presenting patients. The appropriateness of prescribing rather than prescribing rates, therefore, should be used to determine quality.
Keywords: antibiotics; drug prescribing; infectious disease; out-of-hours service; prescribing quality; primary care.
© British Journal of General Practice 2017.
Figures
References
-
- Dekker AR, Verheij TJ, van der Velden AW. Inappropriate antibiotic prescription for respiratory tract indications: most prominent in adult patients. Fam Pract. 2015;32(4):401–407. - PubMed
-
- Shapiro DJ, Hicks LA, Pavia AT, Hersh AL. Antibiotic prescribing for adults in ambulatory care in the USA, 2007–09. J Antimicrob Chemother. 2014;69(1):234–240. - PubMed
-
- Van den Broek d’Obrenan J, Verheij TJ, Numans ME, van der Velden AW. Antibiotic use in Dutch primary care: relation between diagnosis, consultation and treatment. J Antimicrob Chemother. 2014;69(6):1701–1707. - PubMed
-
- Willems CS, van den Broek D’Obrenan J, Numans ME, et al. Cystitis: antibiotic prescribing, consultation, attitudes and opinions. Fam Pract. 2014;31(2):149–155. - PubMed
-
- Costelloe C, Metcalfe C, Lovering A, et al. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical