

Access to Kidney Transplantation among HIV-Infected Waitlist Candidates
- PMID: 28232406
- PMCID: PMC5338712
- DOI: 10.2215/CJN.07460716
Access to Kidney Transplantation among HIV-Infected Waitlist Candidates
Abstract
Background and objectives: Kidney transplantation among HIV-infected patients with ESRD confers a significant survival benefit over remaining on dialysis. Given the high mortality burden associated with dialysis, understanding access to kidney transplantation after waitlisting among HIV+ candidates is warranted.
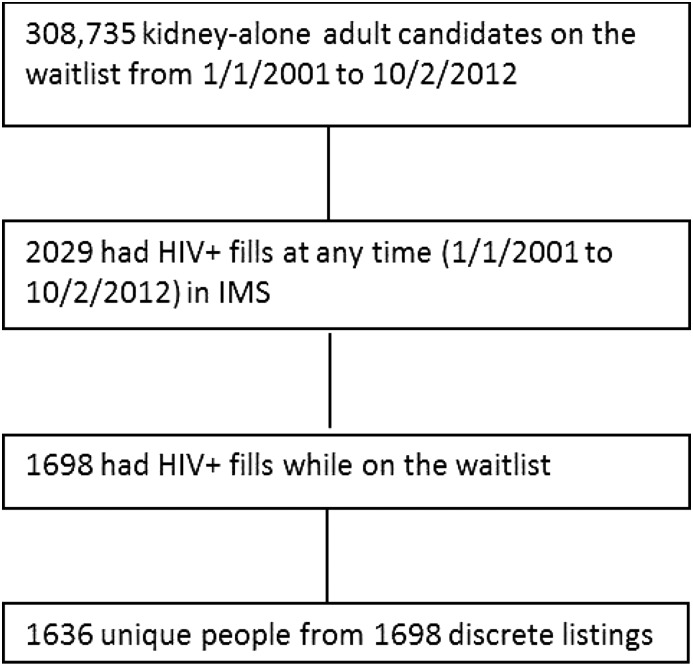
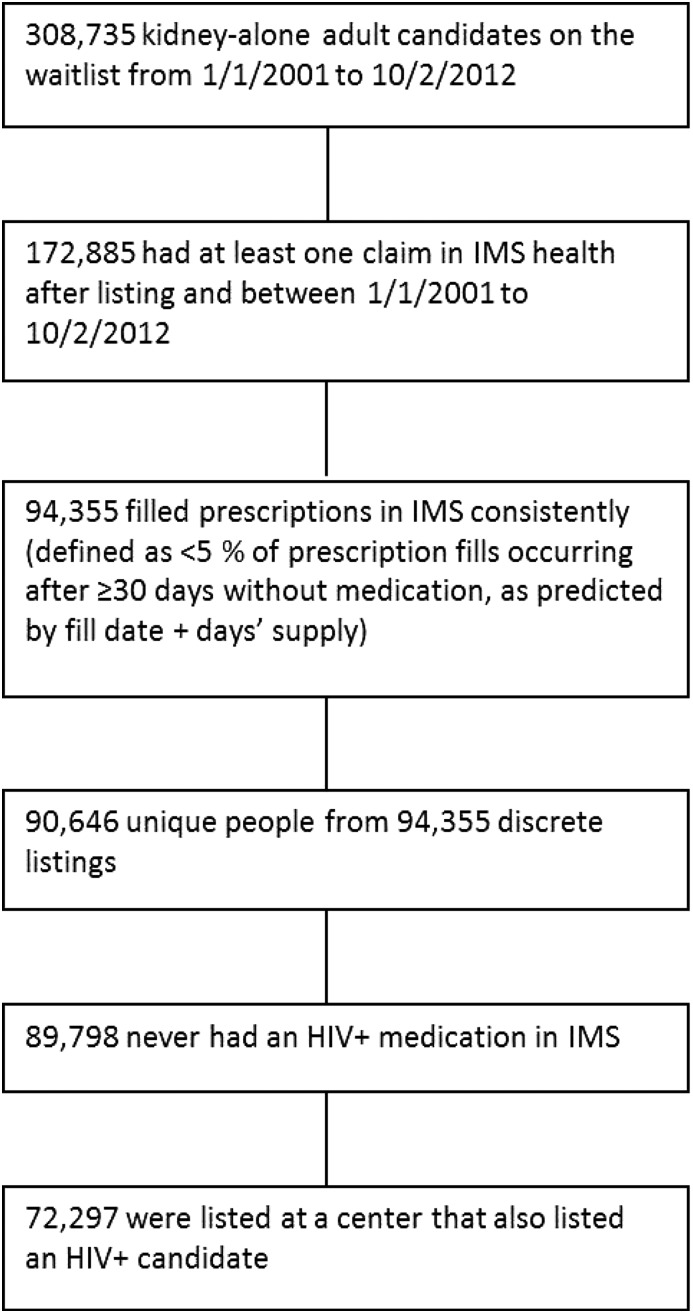
Design, setting, participants, & measurements: Data from the Scientific Registry of Transplant Recipients were linked to Intercontinental Marketing Statistics pharmacy fills (January 1, 2001 to October 1, 2012) so that we could identify and study 1636 HIV+ (defined as having filled one or more antiretroviral medications unique to HIV treatment) and 72,297 HIV- kidney transplantation candidates.
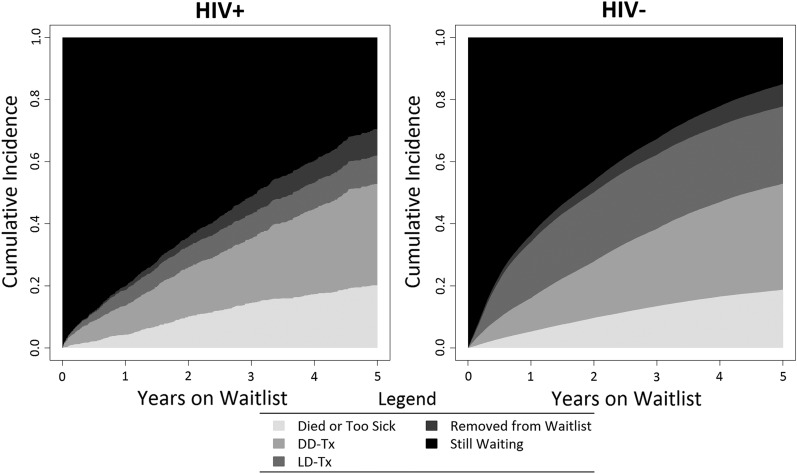
Results: HIV+ waiting list candidates were more often young (<50 years old: 62.7% versus 37.6%; P<0.001), were more often men (75.2% versus 59.3%; P<0.001), were more often black (73.6% versus 27.9%; P<0.001), had longer time on dialysis (years: 2.5 versus 0.8; P<0.001), were more often coinfected with hepatitis C virus (9.0% versus 3.9%; P<0.001), and were less likely to remain active on the waiting list (37.7% versus 49.4%; P<0.001). Waitlist mortality among HIV+ candidates was similar compared with HIV- candidates (adjusted hazard ratio, 1.03; 95% confidence interval, 0.89 to 1.20; P=0.67). In contrast, likelihood of living donor kidney transplantation was 47% lower (adjusted hazard ratio, 0.53; 95% confidence interval, 0.44 to 0.64; P<0.001), and there was a trend toward lower likelihood of deceased donor kidney transplantation (adjusted hazard ratio, 0.87; 95% confidence interval, 0.74 to 1.01; P=0.07) compared with in HIV- candidates.
Conclusions: Our findings highlight the need for additional study to better understand disparities in access to kidney transplantation, particularly living donor kidney transplantation, among HIV+ kidney waitlist candidates.
Keywords: African Continental Ancestry Group; Coinfection; HIV; HIV Infections; HIV-1; Hepatitis C; Humans; Kidney Failure, Chronic; Living Donors; Male; end-stage renal disease; kidney transplantation; renal dialysis.
Copyright © 2017 by the American Society of Nephrology.
Figures
Comment in
-
Opportunities and Challenges for Kidney Donation from and to HIV-Positive Individuals.Clin J Am Soc Nephrol. 2017 Mar 7;12(3):385-387. doi: 10.2215/CJN.00740117. Epub 2017 Feb 23. Clin J Am Soc Nephrol. 2017. PMID: 28232405 Free PMC article. No abstract available.
References
-
- Johnson AS, Beer L, Sionean C, Hu X, Furlow-Parmley C, Le B, Skarbinski J, Hall HI, Dean HD; Centers for Disease Control and Prevention (CDC) : HIV infection - United States, 2008 and 2010. MMWR Suppl 62: 112–119, 2013 - PubMed
-
- Palella FJ Jr., Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, Aschman DJ, Holmberg SD; HIV Outpatient Study Investigators : Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med 338: 853–860, 1998 - PubMed
-
- Rao TK: Human immunodeficiency virus infection in end-stage renal disease patients. Semin Dial 16: 233–244, 2003 - PubMed
-
- Szczech LA, Gange SJ, van der Horst C, Bartlett JA, Young M, Cohen MH, Anastos K, Klassen PS, Svetkey LP: Predictors of proteinuria and renal failure among women with HIV infection. Kidney Int 61: 195–202, 2002 - PubMed
-
- Winston JA, Klotman PE: Are we missing an epidemic of HIV-associated nephropathy? J Am Soc Nephrol 7: 1–7, 1996 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
