

Intracranial and Extracranial Neurovascular Manifestations of Takayasu Arteritis
- PMID: 28232496
- PMCID: PMC7960250
- DOI: 10.3174/ajnr.A5095
Intracranial and Extracranial Neurovascular Manifestations of Takayasu Arteritis
Abstract
Background and purpose: Takayasu arteritis is a rare, large-vessel vasculitis that presents with symptoms related to end-organ ischemia. While the extracranial neurovascular manifestations of Takayasu arteritis are well-established, little is known regarding the intracranial manifestations. In this study, we characterize the intracranial and cervical neurovascular radiologic findings in patients with Takayasu arteritis.
Materials and methods: Patients with Takayasu arteritis who presented to our institution between 2001 and 2016 with intracranial and/or cervical vascular imaging were included in this study. Images were evaluated for the presence of vascular abnormalities, including intracranial or extracranial stenosis, vessel-wall thickening, dissection, subclavian steal, aneurysms, infarcts, and hemorrhages. Descriptive analyses are reported.
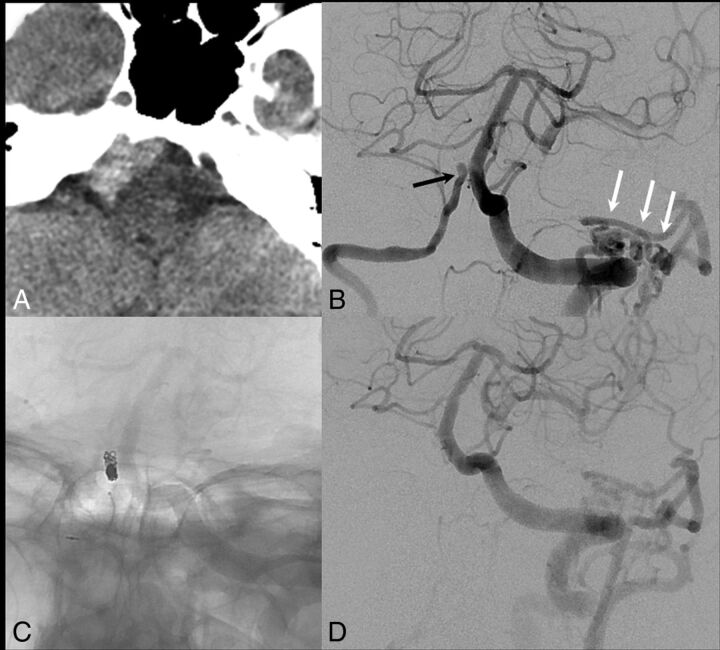
Results: Seventy-nine patients with Takayasu arteritis met the criteria for inclusion in this study. The most common presenting neurologic symptoms were headache (32.9%) and dizziness (15.2%). Intracranial and extracranial vascular imaging was performed in 84.8% and 89.9% of patients, respectively. Among patients with intracranial vascular imaging, 3 (3.9%) had intracranial aneurysms, 3 (3.9%) had acute large-vessel occlusion, 6 (7.6%) had intracranial vasculitis, and 1 (1.3%) had reversible cerebrovascular constriction syndrome. Among patients with cervical vascular imaging, 42 (53.1%) had some degree of narrowing of the common carotid artery and 18 (22.8%) had narrowing of the ICAs. Seventeen patients (23.6%) had subclavian steal.
Conclusions: Intracranial vascular abnormalities in patients with Takayasu arteritis presenting with neurologic symptoms are not rare, with cerebral vasculitis seen in 7.8% of patients, and stroke secondary to large-vessel occlusion, in 3.9% of patients. Cervical vascular manifestations of Takayasu arteritis were present in most patients in our study.
© 2017 by American Journal of Neuroradiology.
Figures



Similar articles
-
Complete ophthalmoplegia, complete ptosis and dilated pupil due to internal carotid artery dissection: as the first manifestation of Takayasu arteritis.BMC Cardiovasc Disord. 2017 Jul 25;17(1):201. doi: 10.1186/s12872-017-0638-7. BMC Cardiovasc Disord. 2017. PMID: 28743241 Free PMC article.
-
Cerebrovascular manifestations of Takayasu arteritis in Europe.Rheumatology (Oxford). 2005 Aug;44(8):1012-5. doi: 10.1093/rheumatology/keh664. Epub 2005 Apr 19. Rheumatology (Oxford). 2005. PMID: 15840603
-
Imaging diagnosis of subclavian steal syndrome secondary to Takayasu arteritis affecting a left-side subclavian artery.Arch Med Res. 2003 Sep-Oct;34(5):433-8. doi: 10.1016/j.arcmed.2003.06.002. Arch Med Res. 2003. PMID: 14602512
-
Takayasu arteritis presenting as epileptic seizures: a case report and brief review of the literature.Rheumatol Int. 2009 Apr;29(6):703-5. doi: 10.1007/s00296-008-0747-9. Epub 2008 Oct 22. Rheumatol Int. 2009. PMID: 18941753 Review.
-
Beyond Giant Cell Arteritis and Takayasu's Arteritis: Secondary Large Vessel Vasculitis and Vasculitis Mimickers.Curr Rheumatol Rep. 2020 Nov 7;22(12):88. doi: 10.1007/s11926-020-00965-w. Curr Rheumatol Rep. 2020. PMID: 33159612 Review.
Cited by
-
Predicting stroke and myocardial infarction risk in Takayasu arteritis with automated machine learning models.iScience. 2023 Nov 9;26(12):108421. doi: 10.1016/j.isci.2023.108421. eCollection 2023 Dec 15. iScience. 2023. PMID: 38077132 Free PMC article.
-
Carotid Artery Stenosis and Ischemic Strokes in Patients with Giant Cell Arteritis: A Characteristic Pattern-Literature Review and Case Report.TH Open. 2021 Nov 23;6(1):e40-e49. doi: 10.1055/a-1704-0741. eCollection 2022 Jan. TH Open. 2021. PMID: 35112048 Free PMC article. Review.
-
Restoration of vision by endovascular revascularization in Takayasu arteritis: A case series.J Cardiol Cases. 2018 Jul 12;18(4):123-127. doi: 10.1016/j.jccase.2018.05.013. eCollection 2018 Oct. J Cardiol Cases. 2018. PMID: 30279928 Free PMC article.
-
Takayasu arteritis: A rare cause of chronic headache.Clin Case Rep. 2021 Sep 21;9(9):e04860. doi: 10.1002/ccr3.4860. eCollection 2021 Sep. Clin Case Rep. 2021. PMID: 34584719 Free PMC article.
-
Basilar Tip Aneurysm in Takayasu Arteritis.BJR Case Rep. 2019 Nov 15;5(4):20180114. doi: 10.1259/bjrcr.20180114. eCollection 2019 Dec. BJR Case Rep. 2019. PMID: 31938555 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous