

Mesenchymal Stem Cells Support Survival and Proliferation of Primary Human Acute Myeloid Leukemia Cells through Heterogeneous Molecular Mechanisms
- PMID: 28232835
- PMCID: PMC5299032
- DOI: 10.3389/fimmu.2017.00106
Mesenchymal Stem Cells Support Survival and Proliferation of Primary Human Acute Myeloid Leukemia Cells through Heterogeneous Molecular Mechanisms
Abstract
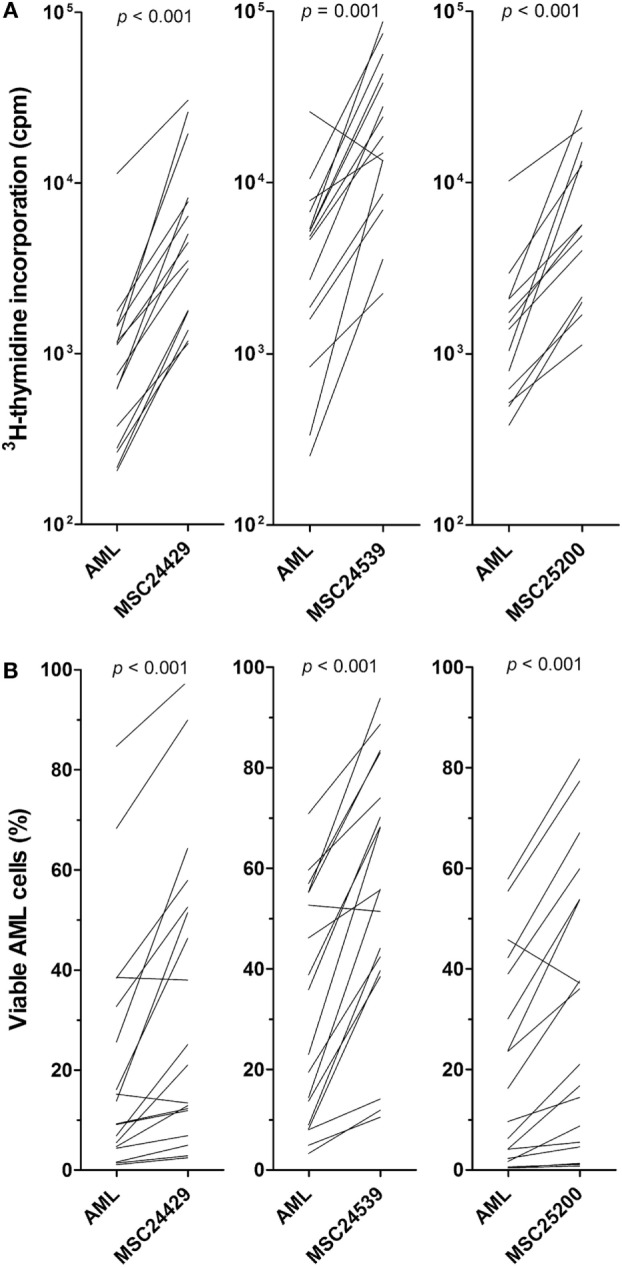
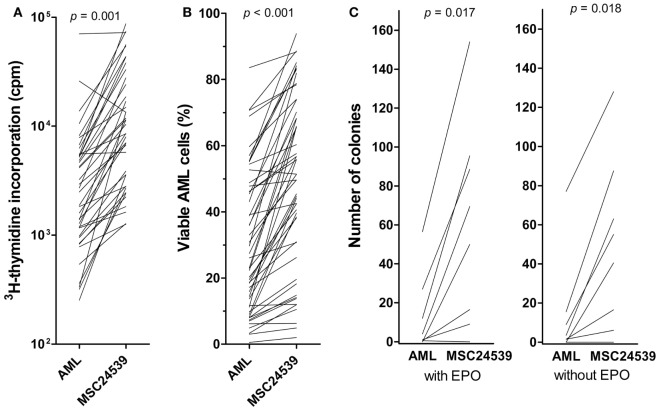
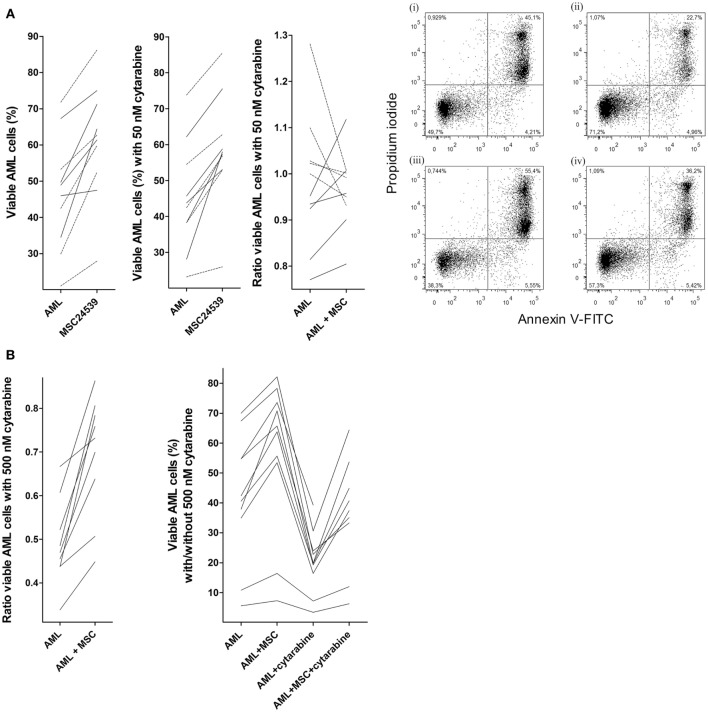
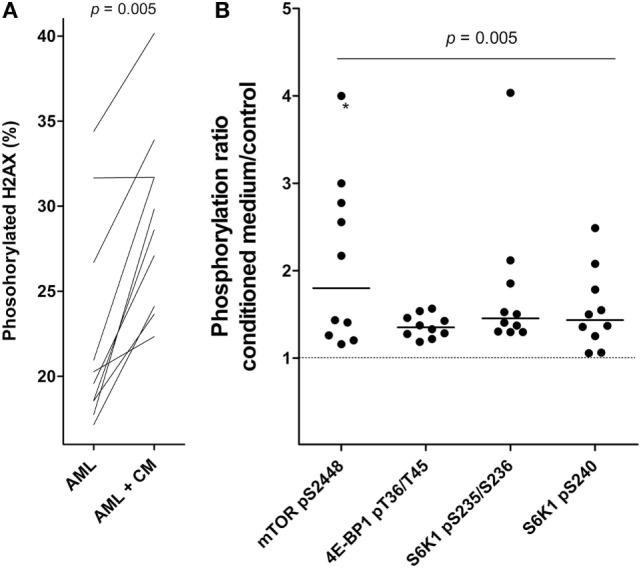
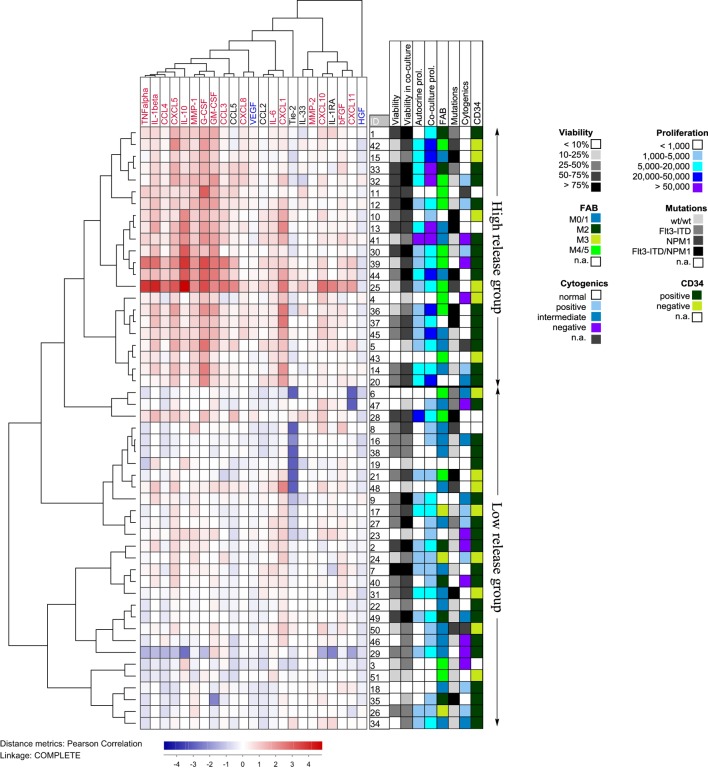
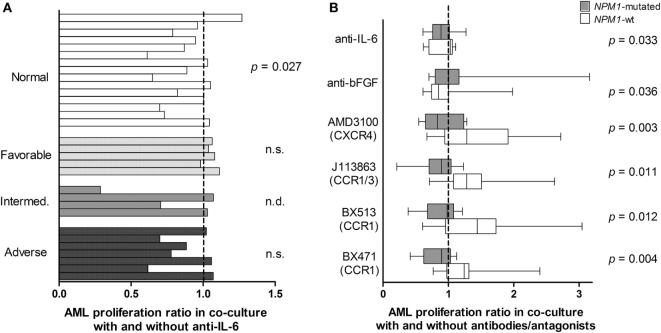
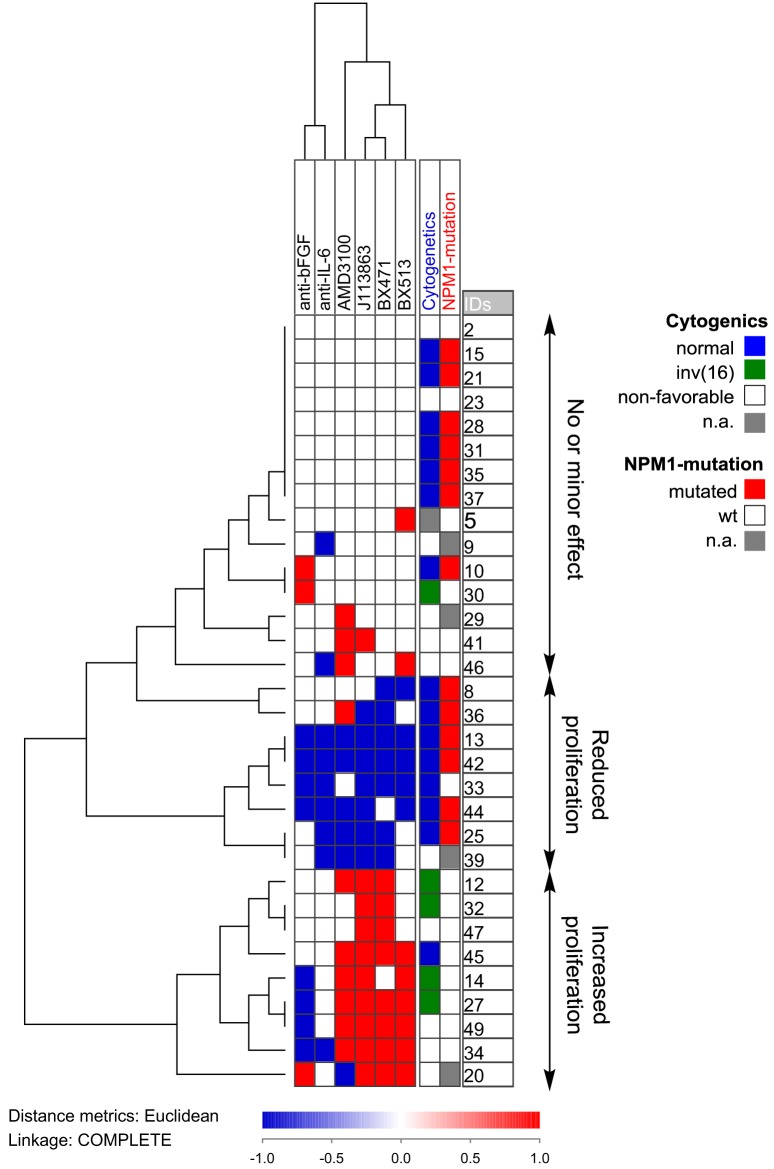
Acute myeloid leukemia (AML) is a bone marrow malignancy, and various bone marrow stromal cells seem to support leukemogenesis, including osteoblasts and endothelial cells. We have investigated how normal bone marrow mesenchymal stem cells (MSCs) support the in vitro proliferation of primary human AML cells. Both MSCs and primary AML cells show constitutive release of several soluble mediators, and the mediator repertoires of the two cell types are partly overlapping. The two cell populations were cocultured on transwell plates, and MSC effects on AML cells mediated through the local cytokine/soluble mediator network could thus be evaluated. The presence of normal MSCs had an antiapoptotic and growth-enhancing effect on primary human AML cells when investigating a group of 51 unselected AML patients; this was associated with increased phosphorylation of mTOR and its downstream targets, and the effect was independent of cytogenetic or molecular-genetic abnormalities. The MSCs also supported the long-term proliferation of the AML cells. A subset of the patients also showed an altered cytokine network with supra-additive levels for several cytokines. The presence of cytokine-neutralizing antibodies or receptor inhibitors demonstrated that AML cells derived from different patients were heterogeneous with regard to effects of various cytokines on AML cell proliferation or regulation of apoptosis. We conclude that even though the effects of single cytokines derived from bone marrow MSCs on human AML cells differ among patients, the final cytokine-mediated effects of the MSCs during coculture is growth enhancement and inhibition of apoptosis.
Keywords: acute myeloid leukemia; apoptosis; chemokines; cytokines; mesenchymal stem cells; proliferation.
Figures
Similar articles
-
The cytokine-mediated crosstalk between primary human acute myeloid cells and mesenchymal stem cells alters the local cytokine network and the global gene expression profile of the mesenchymal cells.Stem Cell Res. 2015 Nov;15(3):530-541. doi: 10.1016/j.scr.2015.09.008. Epub 2015 Sep 25. Stem Cell Res. 2015. PMID: 26468600
-
Microvascular endothelial cells increase proliferation and inhibit apoptosis of native human acute myelogenous leukemia blasts.Int J Cancer. 2006 Nov 15;119(10):2313-21. doi: 10.1002/ijc.22180. Int J Cancer. 2006. PMID: 16921487
-
[Immunomodulatory effects of mesenchymal stem cells derived from the bone marrow in acute leukemia patients].Zhonghua Zhong Liu Za Zhi. 2011 Feb;33(2):105-9. Zhonghua Zhong Liu Za Zhi. 2011. PMID: 21575477 Chinese.
-
The angioregulatory cytokine network in human acute myeloid leukemia - from leukemogenesis via remission induction to stem cell transplantation.Eur Cytokine Netw. 2012 Oct-Dec;23(4):140-53. doi: 10.1684/ecn.2012.0322. Eur Cytokine Netw. 2012. PMID: 23328436 Review.
-
Toll-like Receptor 4, Osteoblasts and Leukemogenesis; the Lesson from Acute Myeloid Leukemia.Molecules. 2022 Jan 23;27(3):735. doi: 10.3390/molecules27030735. Molecules. 2022. PMID: 35163998 Free PMC article. Review.
Cited by
-
Vitamin D Receptor Antagonist MeTC7 Inhibits PD-L1.Cancers (Basel). 2023 Jun 30;15(13):3432. doi: 10.3390/cancers15133432. Cancers (Basel). 2023. PMID: 37444542 Free PMC article.
-
Myeloid-Derived Suppressor Cells and Mesenchymal Stem/Stromal Cells in Myeloid Malignancies.J Clin Med. 2021 Jun 24;10(13):2788. doi: 10.3390/jcm10132788. J Clin Med. 2021. PMID: 34202907 Free PMC article. Review.
-
The constitutive protease release by primary human acute myeloid leukemia cells.J Cancer Res Clin Oncol. 2017 Oct;143(10):1985-1998. doi: 10.1007/s00432-017-2458-7. Epub 2017 Jun 19. J Cancer Res Clin Oncol. 2017. PMID: 28631213 Free PMC article.
-
Mesenchymal stem cells in the bone marrow microenvironment: a double-edged sword for AML.J Cancer Res Clin Oncol. 2025 Jun 21;151(6):193. doi: 10.1007/s00432-025-06244-4. J Cancer Res Clin Oncol. 2025. PMID: 40542231 Free PMC article. Review.
-
Isolation, Maintenance and Expansion of Adult Hematopoietic Stem/Progenitor Cells and Leukemic Stem Cells.Cancers (Basel). 2022 Mar 28;14(7):1723. doi: 10.3390/cancers14071723. Cancers (Basel). 2022. PMID: 35406494 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous