

Higher-risk mitral valve operations after previous sternotomy: endoscopic, minimally invasive approach improves patient outcomes
- PMID: 28234615
- PMCID: PMC5125922
- DOI: 10.1503/cjs.004516
Higher-risk mitral valve operations after previous sternotomy: endoscopic, minimally invasive approach improves patient outcomes
Abstract
Background: Reoperative mitral valve (MV) surgery is associated with significant morbidity and mortality; however, endoscopic minimally invasive surgical techniques may preserve the surgical benefits of conventional mitral operations while potentially reducing perioperative risk and length of stay (LOS) in hospital.
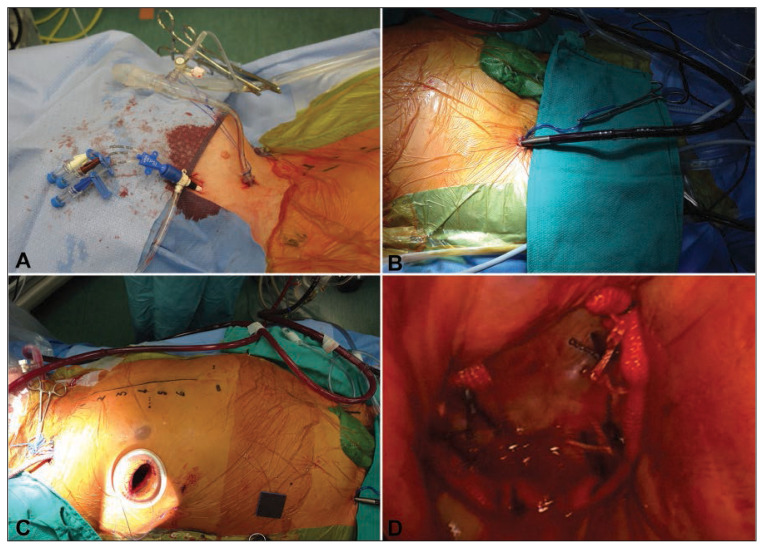
Methods: We compared the outcomes of consecutive patients who underwent reoperative MV surgery between 2000 and 2014 using a minimally invasive endoscopic approach (MINI) with those of patients who underwent a conventional sternotomy (STERN). The primary outcome was in-hospital/30-day mortality. Secondary outcomes included blood product transfusion, LOS in hospital and in the intensive care unit (ICU), and postoperative complications.
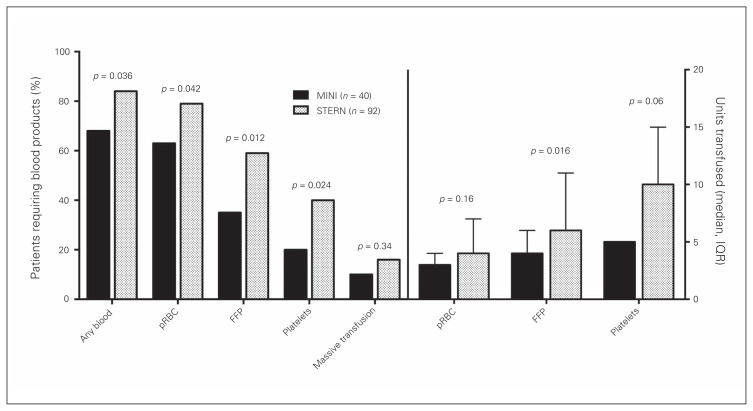
Results: We included 132 patients in our study: 40 (mean age 68 ± 14 yr, 70% men) underwent MINI and 92 (62 ± 13 yr, 40% men) underwent STERN. The MINI group had significantly more comorbidities than the STERN group. While there were no significant differences in complications, all point estimates suggested lower mortality and morbidity in the MINI than the STERN group (in-hospital/ 30-day mortality 5% v. 11%, p = 0.35; composite any of 10 complications 28% v. 41%, p = 0.13). Individual complication rates were similar between the MINI and STERN groups, except for intra-aortic balloon pump requirement (IABP; 0% v. 12%, p = 0.034). MINI significantly reduced the need for any blood transfusion (68% v. 84%, p = 0.036) or packed red blood cells (63% v. 79%, p = 0.042), fresh frozen plasma (35% v. 59%, p = 0.012) and platelets (20% v. 40%, p = 0.024). It also significantly reduced median hospital LOS (8 v. 12 d, p = 0.014). An exploratory propensity score analysis similarly demonstrated a significantly reduced need for IABP (p < 0.001) and a shorter mean LOS in the ICU (p = 0.046) and in hospital (p = 0.047) in the MINI group.
Conclusion: A MINI approach for reoperative MV surgery reduces blood product utilization and hospital LOS. Possible clinically relevant differences in perioperative complications require assessment in randomized clinical trials.
Contexte: Les réopérations de la valve mitrale (VM) sont associées à une morbidité et à une mortalité importantes. Cependant, il semblerait que les techniques chirurgicales endoscopiques à effraction minimale préservent les avantages des opérations traditionnelles de la VM tout en réduisant potentiellement les risques périopératoires et la durée d’hospitalisation.
Méthodes: Nous avons comparé les résultats de patients consécutifs ayant subi une réopération de la VM entre 2000 et 2014 selon une approche endoscopique à effraction minimale (groupe MINI) à ceux de patients ayant subi une sternotomie classique (groupe STERN). Le résultat primaire à l’étude était la mortalité intrahospitalière ou dans les 30 premiers jours, et les résultats secondaires, la transfusion de produits sanguins, la durée du séjour à l’hôpital et à l’unité des soins intensifs (USI), ainsi que les complications postopératoires.
Résultats: Nous avons retenu 132 patients : 40 (âge moyen de 68 ± 14 ans, 70 % d’hommes) dans le groupe MINI et 92 (âge moyen de 62 ± 13 ans, 40 % d’hommes) dans le groupe STERN. Les patients du groupe MINI présentaient un nombre significativement plus élevé de comorbidités que ceux du groupe STERN. Aucune différence significative n’a été observée quant aux complications, mais toutes les estimations ponctuelles pointaient vers une mortalité et une morbidité moindres dans le groupe MINI (mortalité intrahospitalière ou dans les 30 premiers jours : 5 % c. 11 %, p = 0,35; morbidité combinée à la présence d’au moins une complication parmi 10 possibles : 28 % c. 41 %, p = 0,13). Les taux de complications individuels étaient semblables chez les patients des 2 groupes, sauf pour l’exigence de ballon de contrepulsion intra-aortique (BCIA; 0 % c. 12 %, p = 0,034). L’approche MINI a réduit significativement le taux de transfusion de sang (68 % c. 84 %, p = 0,036) ou de concentrés de globules rouges (63 % c. 79 %, p = 0,042), de plasma frais congelé (35 % c. 59 %, p = 0,012) et de plaquettes (20 % c. 40 %, p = 0,024), en plus de diminuer significativement la durée médiane d’hospitalisation (8 jours c. 12 jours, p = 0,014). En outre, une analyse exploratoire du score de propension a révélé une réduction significative du BCIA (p < 0,001) ainsi qu’une durée moyenne de séjour à l’USI (p = 0,046) et à l’hôpital (p = 0,047) plus courte dans le groupe MINI.
Conclusion: Le recours à l’approche endoscopique à effraction minimale pour les réopérations de la VM diminuerait le recours aux produits sanguins et la durée d’hospitalisation. En ce qui a trait aux complications périopératoires, il faudra procéder à des essais cliniques aléatoires pour évaluer les différences possiblement pertinentes sur le plan clinique.
Figures
References
-
- Akins CW, Buckley MJ, Daggett WM, et al. Risk of reoperative valve replacement for failed mitral and aortic bioprostheses. Ann Thorac Surg. 1998;65:1545–51. - PubMed
-
- Jamieson WR, Burr LH, Miyagishima RT, et al. Reoperation for bioprosthetic mitral structural failure: risk assessment. Circulation. 2003;108:II98–102. - PubMed
-
- Elahi M, Dhannapuneni R, Firmin R, et al. Direct complications of repeat median sternotomy in adults. Asian Cardiovasc Thorac Ann. 2005;13:135–8. - PubMed
-
- Macmanus Q, Okies JE, Phillips SJ, et al. Surgical considerations in patients undergoing repeat median sternotomy. J Thorac Cardiovasc Surg. 1975;69:138–43. - PubMed
-
- Dobell AR, Jain AK. Catastrophic hemorrhage during redo sternotomy. Ann Thorac Surg. 1984;37:273–8. - PubMed