

The Role of Microglia in the Etiology and Evolution of Chronic Traumatic Encephalopathy
- PMID: 28234788
- PMCID: PMC5555778
- DOI: 10.1097/SHK.0000000000000859
The Role of Microglia in the Etiology and Evolution of Chronic Traumatic Encephalopathy
Abstract
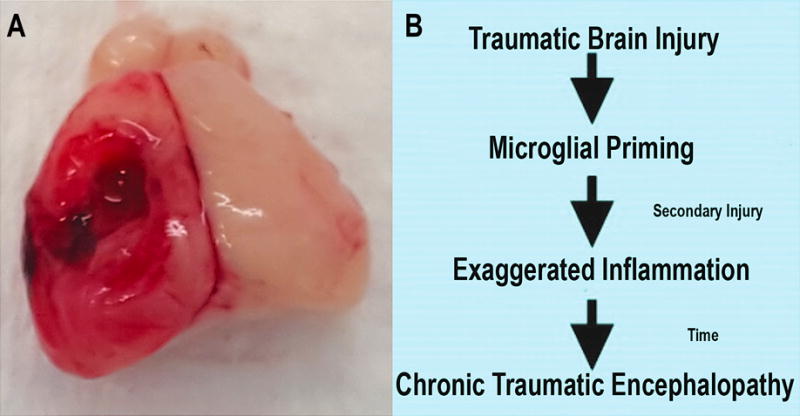
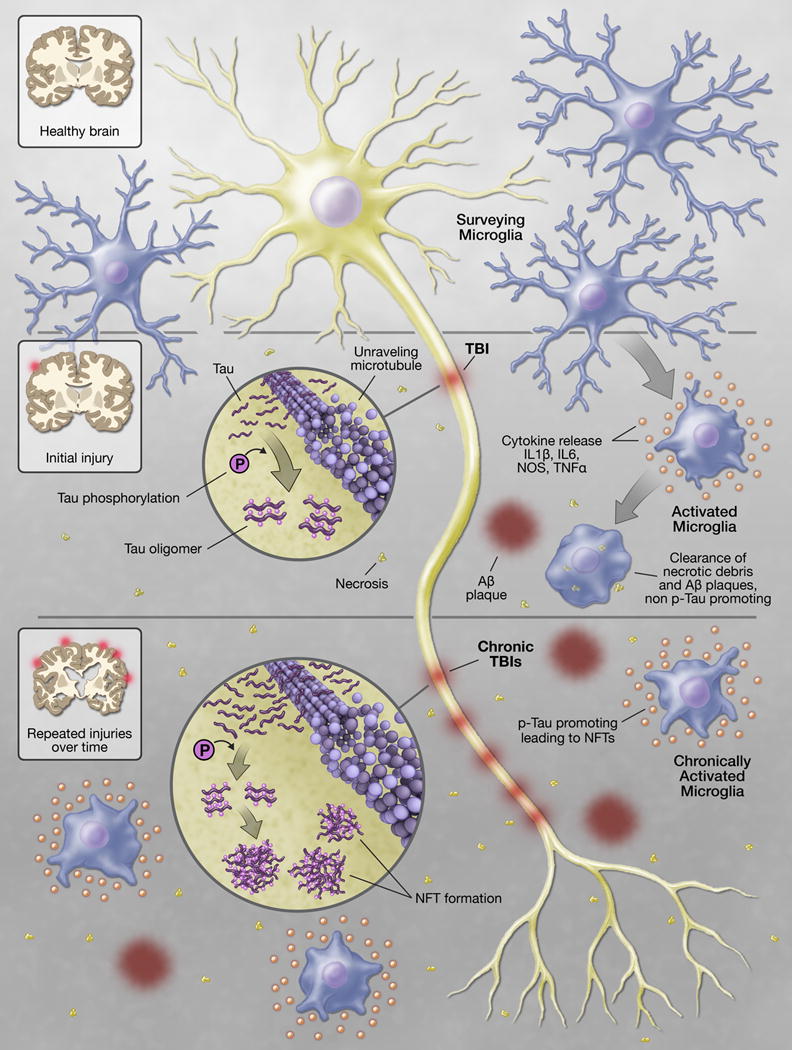
Chronic traumatic encephalopathy (CTE) is a progressive neurodegenerative disease that presents as a late sequela from traumatic brain injury (TBI). TBI is a growing and under-recognized public health concern with a high degree of morbidity and large associated global costs. While the immune response to TBI is complex, its contribution to the development of CTE remains largely unknown. In this review, we summarize the current understanding of the link between CTE and the resident innate immune system of the brain-microglia. We discuss the neuropathology underlying CTE including the creation and aggregation of phosphorylated tau protein into neurofibrillary tangles and the formation of amyloid beta deposits. We also present how microglia, the resident innate immune cells of the brain, drive the continuous low-level inflammation associated with the insidious onset of CTE. In this review, we conclude that the latency period between the index brain injury and the long-term development of CTE presents an opportunity for therapeutic intervention. Encouraging advances with microtubule stabilizers, cis p-tau antibodies, and the ability to therapeutically alter the inflammatory state of microglia have shown positive results in both animal and human trials. Looking forward, recent advancements in next-generation sequencing technology for the study of genomic, transcriptomic, and epigenetic information will provide an opportunity for significant advancement in our understanding of prorepair and pro-injury gene signatures allowing for targeted intervention in this highly morbid injury process.
Figures
References
-
- Faul M. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002–2006. Atlanta (GA): Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2010.
-
- Whitlock JA, Jr, Hamilton BB. Functional outcome after rehabilitation for severe traumatic brain injury. Arch Phys Med Rehabil. 1995;76(12):1103–1112. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
