

Seizure Detection by Critical Care Providers Using Amplitude-Integrated Electroencephalography and Color Density Spectral Array in Pediatric Cardiac Arrest Patients
- PMID: 28234810
- PMCID: PMC5380542
- DOI: 10.1097/PCC.0000000000001099
Seizure Detection by Critical Care Providers Using Amplitude-Integrated Electroencephalography and Color Density Spectral Array in Pediatric Cardiac Arrest Patients
Abstract
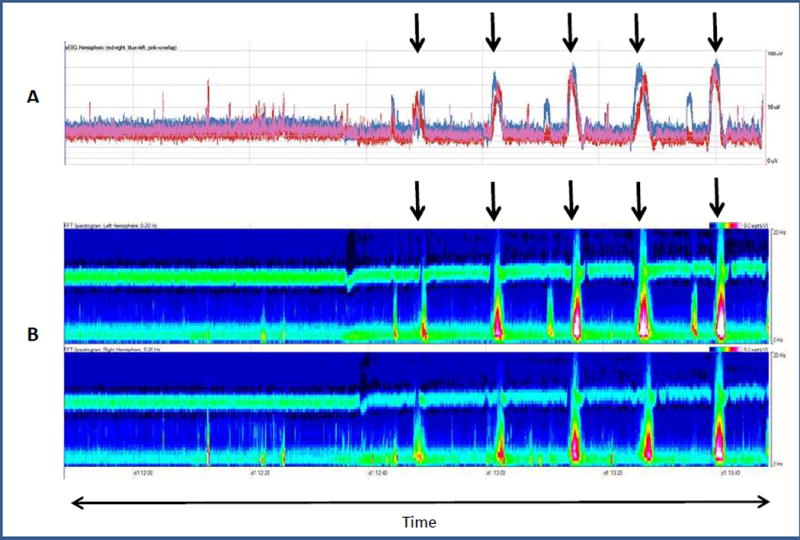
Objectives: Determine the accuracy and confidence of critical care medicine providers to identify seizures using amplitude-integrated electroencephalography versus amplitude-integrated electroencephalography combined with color density spectral array electroencephalography (aEEG + CDSA).
Design: Tutorial and questionnaire.
Setting: PICU.
Subjects: Pediatric critical care providers (attendings, fellows, and nurses).
Interventions: A standardized powerpoint tutorial on amplitude-integrated electroencephalography and color density spectral array followed by classification of 100 amplitude-integrated electroencephalography images and 100 amplitude-integrated electroencephalography combined with color density spectral array as displaying seizures or not displaying seizures.
Measurements and main results: Electroencephalography tracings were obtained from children monitored with continuous electroencephalography after cardiac arrest. The gold standard for seizure identification was continuous electroencephalography interpretation by a pediatric electroencephalographer. The same electroencephalography tracings were used to generate images containing only amplitude-integrated electroencephalography or aEEG + CDSA. Twenty-three critical care medicine providers underwent a 30-minute tutorial on amplitude-integrated electroencephalography and color density spectral array interpretation. They were then asked to determine if there were seizures on 100 amplitude-integrated electroencephalography images and 100 aEEG + CDSA. Amplitude-integrated electroencephalography seizure detection sensitivity was 77% (95% CI, 73%-80%), specificity of 65% (95% CI, 62%-67%), negative predictive value of 88% (95% CI, 86%-90%), and positive predictive value of 46% (95% CI, 43%-49%). For aEEG + CDSA, sensitivity was 77% (95% CI, 74%-81%), specificity of 68% (95% CI, 66%-71%), negative predictive value of 89% (95% CI, 87%-90%), and positive predictive value of 49% (95% CI, 46%-52%). Sensitivity for status epilepticus detection was 77% (95% CI, 71%-82%) with amplitude-integrated electroencephalography and 75% (95% CI, 69%-81%) with aEEG + CDSA. The addition of color density spectral array to amplitude-integrated electroencephalography did not improve seizure detection. However, 87% of critical care medicine providers qualitatively felt that combining both modalities increased their ability to detect seizures.
Conclusions: Amplitude-integrated electroencephalography and aEEG + CDSA offer reasonable sensitivity and negative predictive value for seizure detection by critical care medicine providers. aEEG + CDSA did not improve seizure detection over amplitude-integrated electroencephalography alone although critical care medicine providers felt more confident using both tools combined. Amplitude-integrated electroencephalography and color density spectral array require further evaluation as a tool for screening for seizures and should only be used in conjunction with professional continuous electroencephalography review.
Conflict of interest statement
Conflict of Interest: The authors declare that they have no conflict of interest
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
When the Waves Become Rainbows: Improving Seizure Detection in the Pediatric ICU.Epilepsy Curr. 2018 Mar-Apr;18(2):89-91. doi: 10.5698/1535-7597.18.2.89. Epilepsy Curr. 2018. PMID: 29670484 Free PMC article. No abstract available.
Similar articles
-
Detection of electrographic seizures by critical care providers using color density spectral array after cardiac arrest is feasible.Pediatr Crit Care Med. 2015 Jun;16(5):461-7. doi: 10.1097/PCC.0000000000000352. Pediatr Crit Care Med. 2015. PMID: 25651050 Free PMC article.
-
Seizure Identification by Critical Care Providers Using Quantitative Electroencephalography.Crit Care Med. 2018 Dec;46(12):e1105-e1111. doi: 10.1097/CCM.0000000000003385. Crit Care Med. 2018. PMID: 30188384
-
Detection of seizure patterns with multichannel amplitude-integrated EEG and the color density spectral array in the adult neurology intensive care unit.Medicine (Baltimore). 2018 Sep;97(38):e12514. doi: 10.1097/MD.0000000000012514. Medicine (Baltimore). 2018. PMID: 30235767 Free PMC article. Clinical Trial.
-
Amplitude-integrated electroencephalography for seizure detection in newborn infants.Semin Fetal Neonatal Med. 2018 Jun;23(3):175-182. doi: 10.1016/j.siny.2018.02.003. Epub 2018 Feb 13. Semin Fetal Neonatal Med. 2018. PMID: 29472139 Review.
-
Using amplitude-integrated EEG in neonatal intensive care.J Perinatol. 2010 Oct;30 Suppl:S73-81. doi: 10.1038/jp.2010.93. J Perinatol. 2010. PMID: 20877412 Review.
Cited by
-
Multimodal Neurologic Monitoring in Children With Acute Brain Injury.Pediatr Neurol. 2022 Apr;129:62-71. doi: 10.1016/j.pediatrneurol.2022.01.006. Epub 2022 Feb 2. Pediatr Neurol. 2022. PMID: 35240364 Free PMC article. Review.
-
Neurologic Outcomes Following Care in the Pediatric Intensive Care Unit.Curr Treat Options Pediatr. 2017 Sep;3(3):193-207. doi: 10.1007/s40746-017-0092-x. Epub 2017 Jul 26. Curr Treat Options Pediatr. 2017. PMID: 29218262 Free PMC article.
-
Characterization of aEEG During Sleep and Wakefulness in Healthy Children.Front Pediatr. 2022 Jan 21;9:773188. doi: 10.3389/fped.2021.773188. eCollection 2021. Front Pediatr. 2022. PMID: 35127587 Free PMC article.
-
Competence of healthcare professionals performing electroencephalography test: A systematic review.Clin Neurophysiol Pract. 2025 Mar 8;10:104-115. doi: 10.1016/j.cnp.2025.03.001. eCollection 2025. Clin Neurophysiol Pract. 2025. PMID: 40160931 Free PMC article. Review.
-
The impact of age and electrode position on amplitude-integrated EEGs in children from 1 month to 17 years of age.Front Neurol. 2022 Aug 25;13:952193. doi: 10.3389/fneur.2022.952193. eCollection 2022. Front Neurol. 2022. PMID: 36090865 Free PMC article.
References
-
- Abend NS, Dlugos DJ. Nonconvulsive status epilepticus in a pediatric intensive care unit. Pediatr Neurol. 2007;37(3):165–70. - PubMed
-
- Jette N, Claassen J, Emerson RG. Frequency and predictors of nonconvulsive seizures during continuous electroencephalographic monitoring in critically ill children. Arch Neurol. 2006;63(12):1750–5. - PubMed
-
- Hosain SA, Solomon GE, Kobylarz EJ. Electroencephalographic patterns in unresponsive pediatric patients. Pediatr Neurol. 2005;32(3):162–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
