

Prognostic value of dobutamine stress myocardial perfusion echocardiography in patients with known or suspected coronary artery disease and normal left ventricular function
- PMID: 28234978
- PMCID: PMC5325237
- DOI: 10.1371/journal.pone.0172280
Prognostic value of dobutamine stress myocardial perfusion echocardiography in patients with known or suspected coronary artery disease and normal left ventricular function
Abstract
Objective: We sought to determine the prognostic value of qualitative and quantitative analysis obtained by real-time myocardial perfusion echocardiography (RTMPE) in patients with known or suspected coronary artery disease (CAD).
Background: Quantification of myocardial blood flow reserve (MBFR) in patients with CAD using RTMPE has been demonstrated to further improve accuracy over the analysis of wall motion (WM) and qualitative analysis of myocardial perfusion (QMP).
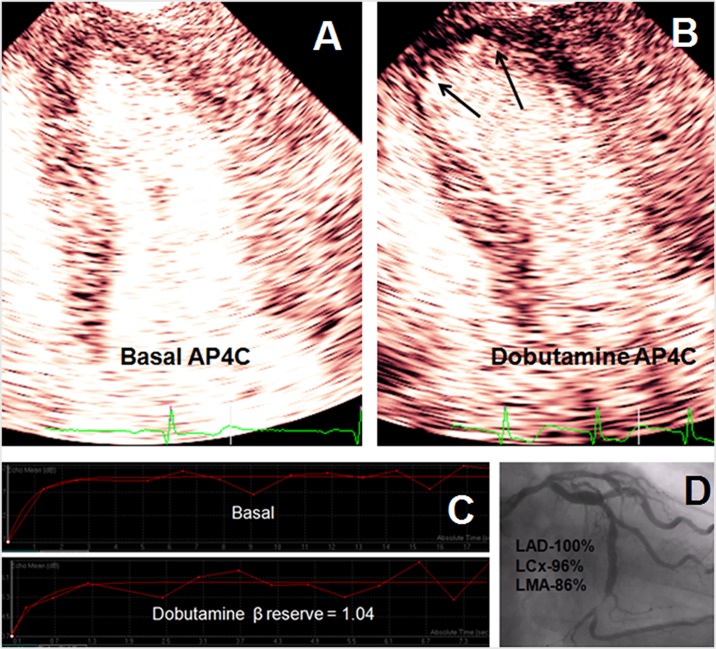
Methods: From March 2003 to December 2008, we prospectively studied 168 patients with normal left ventricular function (LVF) who underwent dobutamine stress RTMPE. The replenishment velocity reserve (β) and MBFR were derived from RTMPE. Acute coronary events were: cardiac death, myocardial infarction and unstable angina with need for urgent coronary revascularization.
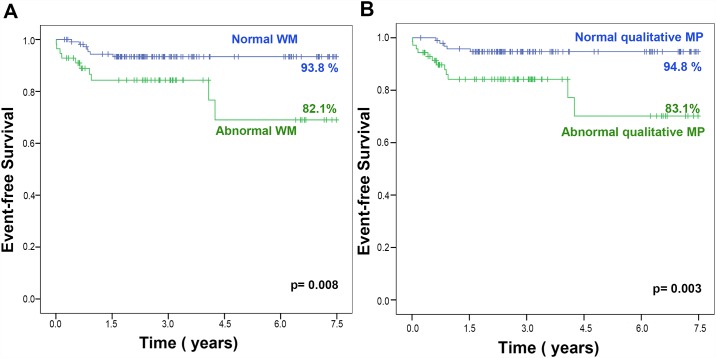
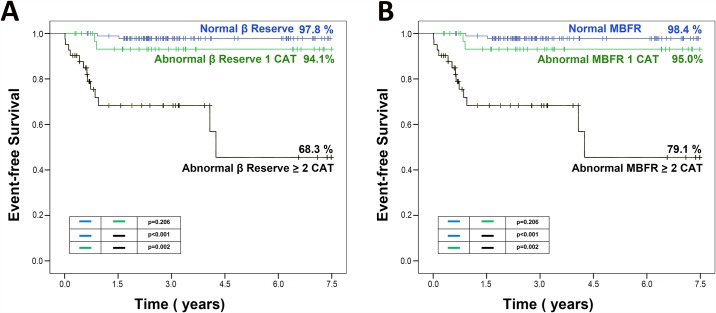
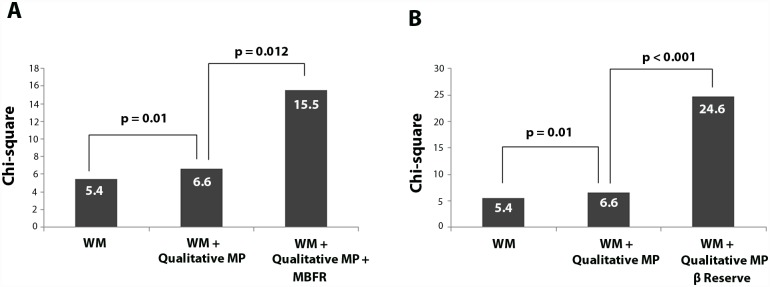
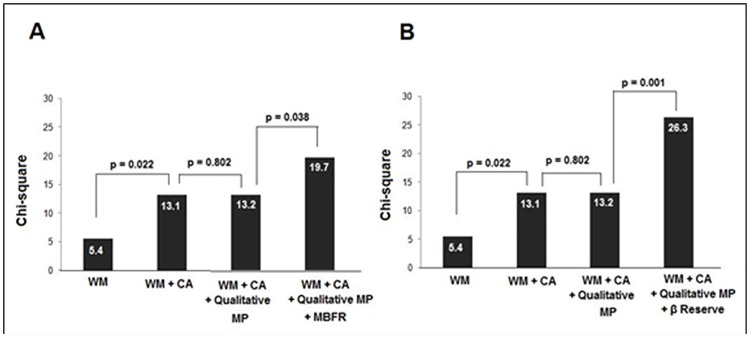
Results: During a median follow-up of 34 months (5 days to 6.9 years), 17 acute coronary events occurred. Abnormal β reserve in ≥2 coronary territories was the only independent predictor of events hazard ratio (HR) = 21, 95% CI = 4.5-99; p<0.001). Both, abnormal β reserve and MBFR added significant incremental value in predicting events over qualitative analysis of WM and MP (χ2 = 6.6 and χ2 = 24.6, respectively; p = 0.001 and χ2 = 6.6 and χ2 = 15.5, respectively; p = 0.012, respectively). When coronary angiographic data was added to the multivariate analysis model, β reserve remained the only predictor of events with HR of 21.0 (95% CI = 4.5-99); p<0.001.
Conclusion: Quantitative dobutamine stress RTMPE provides incremental prognostic information over clinical variables, qualitative analysis of WM and MP, and coronary angiography in predicting acute coronary events.
Conflict of interest statement
Figures
References
-
- Picano E, Mathias W Jr., Pingitore A, Bigi R, Previtali M. Safety and tolerability of dobutamine-atropine stress echocardiography: a prospective, multicentre study. Echo Dobutamine International Cooperative Study Group. Lancet. 1994;344:1190–1992. - PubMed
-
- Mathias W Jr, Tsutsui JM, Andrade JL, Kowatsch I, Lemos PA, Leal SMB, et al. Value of rapid beta-blocker injection at peak dobutamine-atropine stress echocardiography for detection of coronary artery disease. J Am Coll Cardiol. 2003;41:1583–1589. - PubMed
-
- Pingitore A, Picano E, Varga A, Gigli G, Cortigiani L, Previtali M, et al. Prognostic value of pharmacological stress echocardiography in patients with known or suspected coronary artery disease: a prospective, large-scale, multicenter, head-to-head comparison between dipyridamole and dobutamine test. Echo-Persantine International Cooperative (EPIC) and Echo-Dobutamine International Cooperative (EDIC) Study Groups. J Am Coll Cardiol. 1999;34:1769–1777. - PubMed
-
- Wei K, Jayaweera AR, Firoozan S, Linka A, Skyba DM, Kaul S. Quantification of myocardial blood flow with ultrasound-induced destruction of microbubbles administered as a constant venous infusion. Circulation. 1998;97:473–483. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
