

Interrater agreement of two adverse drug reaction causality assessment methods: A randomised comparison of the Liverpool Adverse Drug Reaction Causality Assessment Tool and the World Health Organization-Uppsala Monitoring Centre system
- PMID: 28235001
- PMCID: PMC5325562
- DOI: 10.1371/journal.pone.0172830
Interrater agreement of two adverse drug reaction causality assessment methods: A randomised comparison of the Liverpool Adverse Drug Reaction Causality Assessment Tool and the World Health Organization-Uppsala Monitoring Centre system
Abstract
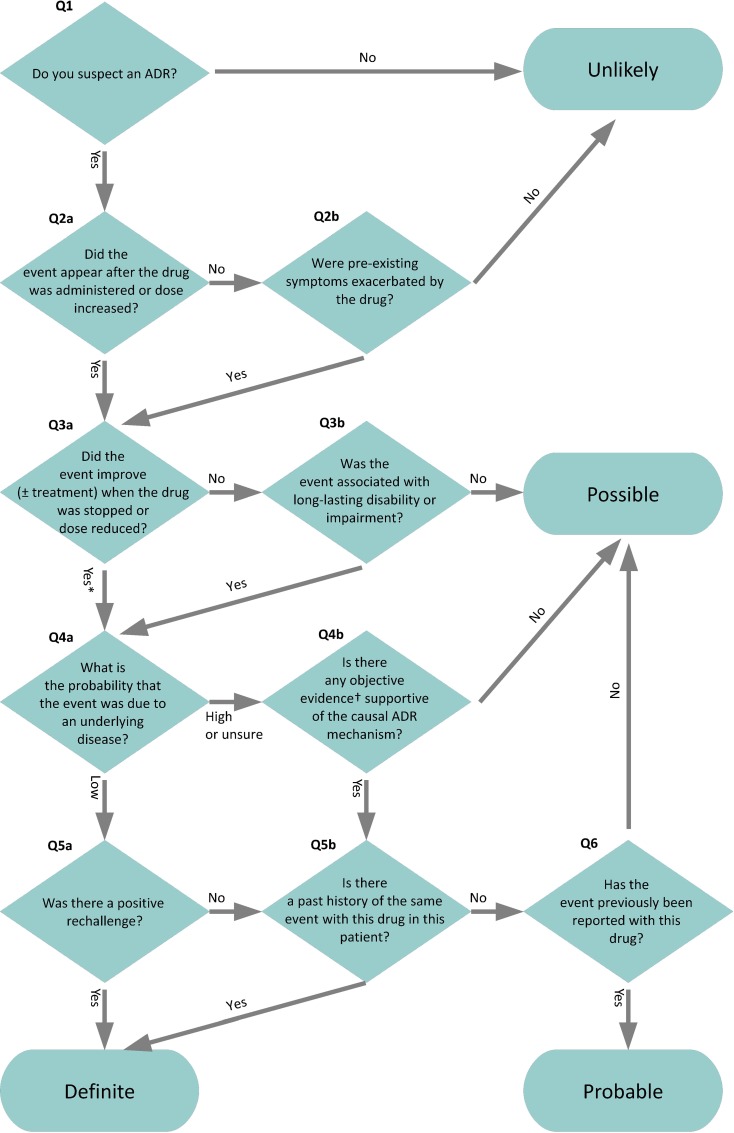
Introduction: A new method to assess causality of suspected adverse drug reactions, the Liverpool Adverse Drug Reaction Causality Assessment Tool (LCAT), showed high interrater agreement when used by its developers. Our aim was to compare the interrater agreement achieved by LCAT to that achieved by another causality assessment method, the World Health Organization-Uppsala Monitoring Centre system for standardised case causality assessment (WHO-UMC system), in our setting.
Methods: Four raters independently assessed adverse drug reaction causality of 48 drug-event pairs, identified during a hospital-based survey. A randomised design ensured that no washout period was required between assessments with the two methods. We compared the methods' interrater agreement by calculating agreement proportions, kappa statistics, and the intraclass correlation coefficient. We identified potentially problematic questions in the LCAT by comparing raters' responses to individual questions.
Results: Overall unweighted kappa was 0.61 (95% CI 0.43 to 0.80) on the WHO-UMC system and 0.27 (95% CI 0.074 to 0.46) on the LCAT. Pairwise unweighted Cohen kappa ranged from 0.33 to 1.0 on the WHO-UMC system and from 0.094 to 0.71 on the LCAT. The intraclass correlation coefficient was 0.86 (95% CI 0.74 to 0.92) on the WHO-UMC system and 0.61 (95% CI 0.39 to 0.77) on the LCAT. Two LCAT questions were identified as significant points of disagreement.
Discussion: We were unable to replicate the high interrater agreement achieved by the LCAT developers and instead found its interrater agreement to be lower than that achieved when using the WHO-UMC system. We identified potential reasons for this and recommend priority areas for improving the LCAT.
Conflict of interest statement
Figures
Similar articles
-
Inter-rater agreement between WHO- Uppsala Monitoring Centre system and Naranjo algorithm for causality assessment of adverse drug reactions.J Pharmacol Toxicol Methods. 2024 May-Jun;127:107514. doi: 10.1016/j.vascn.2024.107514. Epub 2024 May 18. J Pharmacol Toxicol Methods. 2024. PMID: 38768933
-
Comparison of WHO-UMC and Naranjo Scales for Causality Assessment of Reported Adverse Drug Reactions.J Patient Saf. 2024 Jun 1;20(4):236-239. doi: 10.1097/PTS.0000000000001213. Epub 2024 Feb 12. J Patient Saf. 2024. PMID: 38345209
-
Comparison of different methods for causality assessment of adverse drug reactions.Int J Clin Pharm. 2018 Aug;40(4):903-910. doi: 10.1007/s11096-018-0694-9. Epub 2018 Jul 26. Int J Clin Pharm. 2018. PMID: 30051231
-
A scoping review of the clinical utility of adverse drug reaction causality analysis tools for use in the hospital setting.Expert Rev Clin Pharmacol. 2024 Dec;17(12):1127-1148. doi: 10.1080/17512433.2024.2429677. Epub 2024 Nov 22. Expert Rev Clin Pharmacol. 2024. PMID: 39535130
-
Evaluation of patient reporting of adverse drug reactions to the UK 'Yellow Card Scheme': literature review, descriptive and qualitative analyses, and questionnaire surveys.Health Technol Assess. 2011 May;15(20):1-234, iii-iv. doi: 10.3310/hta15200. Health Technol Assess. 2011. PMID: 21545758 Review.
Cited by
-
Efficacy of acupuncture at three nasal acupoints plus acupoint application for perennial allergic rhinitis: A multicenter, randomized controlled trial protocol.Trials. 2020 Jan 28;21(1):110. doi: 10.1186/s13063-019-4039-3. Trials. 2020. PMID: 31992367 Free PMC article.
-
Avoidability of drug-induced liver injury (DILI) in an elderly hospital cohort with cases assessed for causality by the updated RUCAM score.BMC Geriatr. 2020 Sep 14;20(1):346. doi: 10.1186/s12877-020-01732-3. BMC Geriatr. 2020. PMID: 32928134 Free PMC article.
-
Study on the Classification, Causality, Preventability and Severity of Adverse Drug Reaction Using Spontaneous Reporting System in Hospitalized Patients.Pharmacy (Basel). 2018 Sep 29;6(4):108. doi: 10.3390/pharmacy6040108. Pharmacy (Basel). 2018. PMID: 30274320 Free PMC article.
-
An investigation into the avoidability of adverse drug reactions using the LAAT and modified Hallas tools.Medicine (Baltimore). 2020 Jan;99(1):e18569. doi: 10.1097/MD.0000000000018569. Medicine (Baltimore). 2020. PMID: 31895800 Free PMC article.
-
Causality and avoidability of adverse drug reactions of antibiotics in hospitalized children: a cohort study.Int J Clin Pharm. 2021 Oct;43(5):1293-1301. doi: 10.1007/s11096-021-01249-8. Epub 2021 Mar 3. Int J Clin Pharm. 2021. PMID: 33656658
References
-
- Agbabiaka TB, Savović J, Ernst E. Methods for causality assessment of adverse drug reactions: a systematic review. Drug Saf. 2008;31:21–37. - PubMed
-
- Uppsala Monitoring Centre. The use of the WHO-UMC system for standardized case causality assessment. Available: http://who-umc.org/Graphics/24734.pdf.
-
- Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239–45. - PubMed
-
- Smyth RL, Peak M, Turner MA, Nunn AJ, Williamson PR, Young B, et al. ADRIC: Adverse Drug Reactions In Children–a programme of research using mixed methods. Programme Grants Appl Res. 2014;2(3). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
