

P53 and Ki-67 as prognostic markers in triple-negative breast cancer patients
- PMID: 28235003
- PMCID: PMC5325264
- DOI: 10.1371/journal.pone.0172324
P53 and Ki-67 as prognostic markers in triple-negative breast cancer patients
Abstract
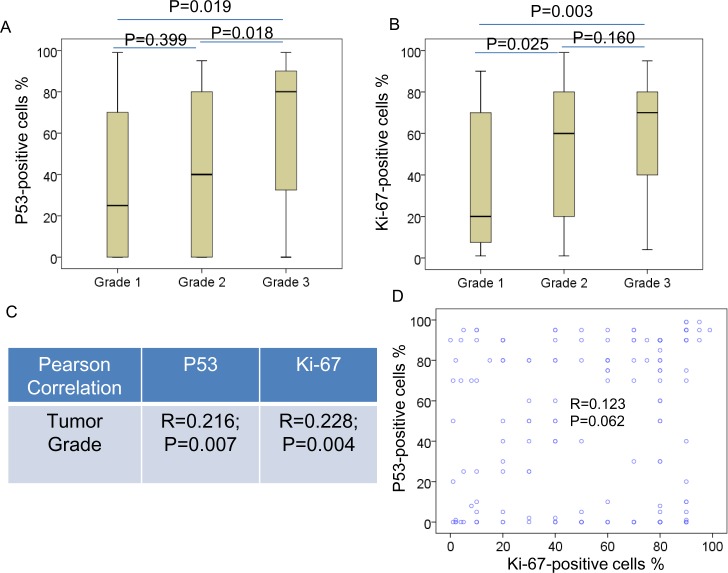
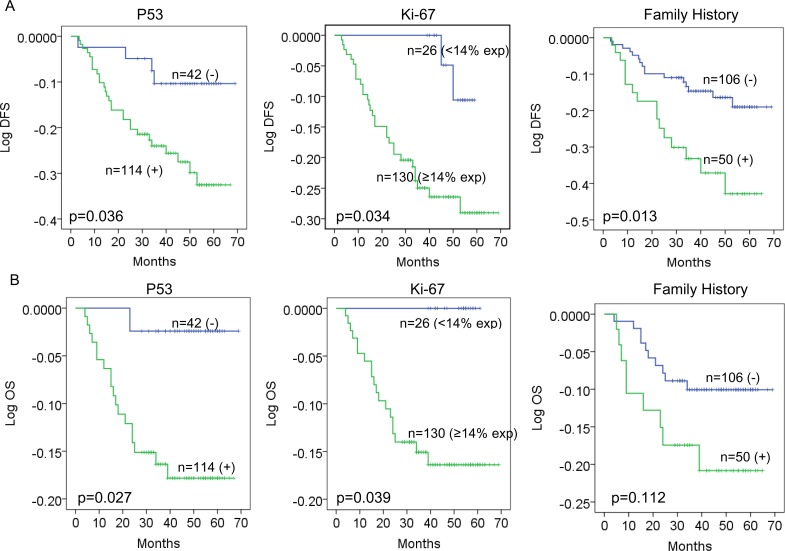
Triple-negative breast cancer (TNBC) is an aggressive subgroup of breast cancer lack of effective target therapy. This study was to investigate the prognostic role of p53 and Ki-67 in 156 cases of TNBC patients. Logistic regression analysis was used to examine the association between clinical parameters and recurrence. Univariate and multivariate analyses were used to examine the association between clinical characteristics and disease-free survival (DFS) or overall survival (OS). Survival analyses using the Kaplan-Meier method were performed to examine the association between p53/Ki-67 and DFS and OS. Our data showed that p53 was positive in 71.3% and the Ki-67 high index was in 82.8% of TNBC. Elevated p53 and Ki-67 were associated with histological grade. The tumor size, lymph node involvement, and p53 expression are associated with risk of recurrence. Tumor size, lymph node involvement, family history, Ki-67 and p53 are independent variables associated with either DFS or OS. TNBC patients with positive p53 or Ki-67 high index or family history of cancer have a significant association with worse prognosis. This study suggests that p53, Ki-67 and family history are useful prognostic markers in TNBC.
Conflict of interest statement
Figures
Similar articles
-
Apoptosis regulator Bcl-2 is an independent prognostic marker for worse overall survival in triple-negative breast cancer patients.Int J Biol Markers. 2018 Jan;33(1):109-115. doi: 10.5301/ijbm.5000291. Int J Biol Markers. 2018. PMID: 28777433
-
Prognostic significance of proline, glutamic acid, leucine rich protein 1 (PELP1) in triple-negative breast cancer: a retrospective study on 129 cases.BMC Cancer. 2015 Oct 15;15:699. doi: 10.1186/s12885-015-1694-y. BMC Cancer. 2015. PMID: 26472563 Free PMC article.
-
Androgen Receptor (AR), E-Cadherin, and Ki-67 as Emerging Targets and Novel Prognostic Markers in Triple-Negative Breast Cancer (TNBC) Patients.PLoS One. 2015 Jun 3;10(6):e0128368. doi: 10.1371/journal.pone.0128368. eCollection 2015. PLoS One. 2015. PMID: 26039245 Free PMC article.
-
Subcellular expression of MTA1, HIF1A and p53 in primary tumor predicts aggressive triple negative breast cancers: a meta-analysis based study.J Mol Histol. 2024 Jun;55(3):303-315. doi: 10.1007/s10735-024-10190-9. Epub 2024 Apr 13. J Mol Histol. 2024. PMID: 38613589
-
Metaplastic Carcinoma of the Breast Is More Aggressive Than Triple-negative Breast Cancer: A Study From a Single Institution and Review of Literature.Clin Breast Cancer. 2017 Aug;17(5):382-391. doi: 10.1016/j.clbc.2017.04.009. Epub 2017 Apr 26. Clin Breast Cancer. 2017. PMID: 28529029 Free PMC article. Review.
Cited by
-
Expression of substance P, neurokinin 1 receptor, Ki-67 and pyruvate kinase M2 in hormone receptor negative breast cancer and evaluation of impact on overall survival.BMC Cancer. 2023 Feb 16;23(1):158. doi: 10.1186/s12885-023-10633-8. BMC Cancer. 2023. PMID: 36797689 Free PMC article.
-
Preclinical Therapeutic Assessment of a New Chemotherapeutics [Dichloro(4,4'-Bis(2,2,3,3-Tetrafluoropropoxy) Methyl)-2,2'-Bipryridine) Platinum] in an Orthotopic Patient-Derived Xenograft Model of Triple-Negative Breast Cancers.Pharmaceutics. 2022 Apr 11;14(4):839. doi: 10.3390/pharmaceutics14040839. Pharmaceutics. 2022. PMID: 35456673 Free PMC article.
-
Are Transcription Factors Plausible Oncotargets for Triple Negative Breast Cancers?Cancers (Basel). 2022 Feb 22;14(5):1101. doi: 10.3390/cancers14051101. Cancers (Basel). 2022. PMID: 35267409 Free PMC article. Review.
-
Naturally-Occurring Canine Mammary Tumors as a Translational Model for Human Breast Cancer.Front Oncol. 2020 Apr 28;10:617. doi: 10.3389/fonc.2020.00617. eCollection 2020. Front Oncol. 2020. PMID: 32411603 Free PMC article. Review.
-
The impact of lipid metabolism on breast cancer: a review about its role in tumorigenesis and immune escape.Cell Commun Signal. 2023 Jun 27;21(1):161. doi: 10.1186/s12964-023-01178-1. Cell Commun Signal. 2023. PMID: 37370164 Free PMC article. Review.
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA: a cancer journal for clinicians. 2015;65(2):87–108. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
