

Increasing body mass index predicts increasing difficulty, failure rate, and time to discovery of failure of epidural anesthesia in laboring patients
- PMID: 28235511
- PMCID: PMC6145168
- DOI: 10.1016/j.jclinane.2016.11.010
Increasing body mass index predicts increasing difficulty, failure rate, and time to discovery of failure of epidural anesthesia in laboring patients
Abstract
Study objective: Obese parturients both greatly benefit from neuraxial techniques, and may represent a technical challenge to obstetric anesthesiologists. Several studies address the topic of obesity and neuraxial analgesia in general, but few offer well described definitions or rates of "difficulty" and "failure" of labor epidural analgesia. Providing those definitions, we hypothesized that increasing body mass index (BMI) is associated with negative outcomes in both categories and increased time needed for epidural placement.
Design: Single center retrospective chart review.
Setting: Labor and Delivery Unit of an inner city academic teaching hospital.
Patients: 2485 parturients, ASA status 2 to 4, receiving labor epidural analgesia for anticipated vaginal delivery.
Interventions: None.
Measurements: We reviewed quality assurance and anesthesia records over a 12-month period. "Failure" was defined as either inadequate analgesia or a positive test dose, requiring replacement, and/or when the anesthesia record stated they failed. "Difficulty" was defined as six or more needle redirections or a note indicating difficulty in the anesthesia record.
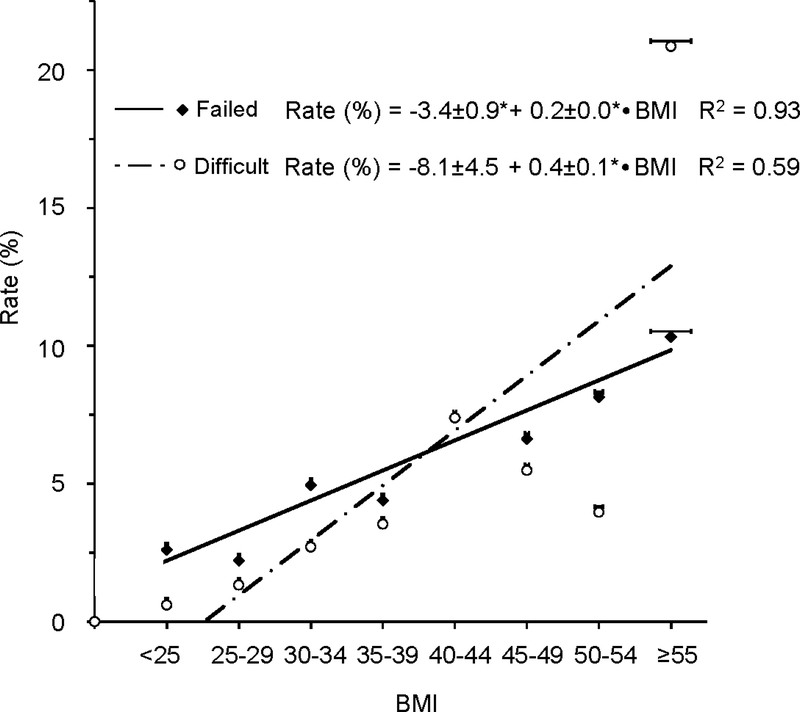
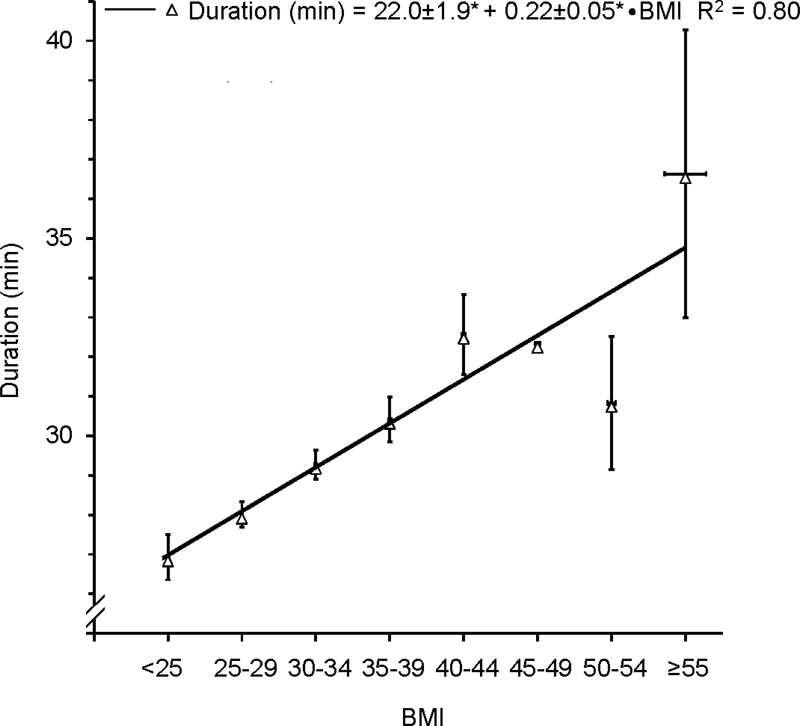
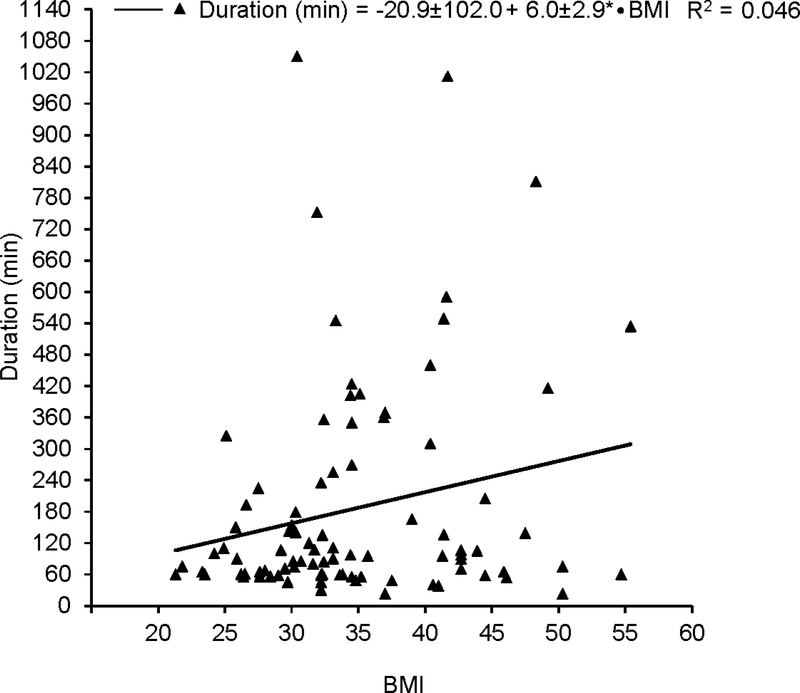
Main results: Overall epidural failure and difficulty rates were 4.3% and 3.0%, respectively. Patients with a BMI of 30kg/m2 or higher had a higher chance of both failure and difficulty with two and almost three fold increases, respectively. Regression analysis indicated that failure was best predicted by BMI and less provider training while difficulty was best predicted by BMI. Additionally, increased BMI was associated with increased time of discovery of epidural catheter failure.
Conclusions: Obesity is associated with increasing technical difficulty and failure of neuraxial analgesia for labor. Practitioners should consider allotting extra time for obese parturients in order to manage potential problems.
Keywords: BMI; Cesarean section; Dural puncture; Inadequate analgesia; Labor epidural; Morbid obesity; Neuraxial; Quality assurance.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The Relationship of Body Mass Index with the Incidence of Postdural Puncture Headache in Parturients.Anesth Analg. 2015 Aug;121(2):451-6. doi: 10.1213/ANE.0000000000000802. Anesth Analg. 2015. PMID: 25993388
-
Incidence and characteristics of failures in obstetric neuraxial analgesia and anesthesia: a retrospective analysis of 19,259 deliveries.Int J Obstet Anesth. 2004 Oct;13(4):227-33. doi: 10.1016/j.ijoa.2004.04.008. Int J Obstet Anesth. 2004. PMID: 15477051
-
Neuraxial labor analgesia failure rates in women with a body mass index ≥50 kg/m2: a single-center retrospective study.Int J Obstet Anesth. 2021 Nov;48:103176. doi: 10.1016/j.ijoa.2021.103176. Epub 2021 May 1. Int J Obstet Anesth. 2021. PMID: 33994271
-
Risk factors for failure of conversion from epidural labor analgesia to cesarean section anesthesia and general anesthesia incidence: an updated meta-analysis.J Matern Fetal Neonatal Med. 2023 Dec;36(2):2278020. doi: 10.1080/14767058.2023.2278020. Epub 2023 Nov 5. J Matern Fetal Neonatal Med. 2023. PMID: 37926901 Review.
-
Modern neuraxial labor analgesia: options for initiation, maintenance and drug selection.Rev Esp Anestesiol Reanim. 2009 Nov;56(9):546-61. doi: 10.1016/s0034-9356(09)70457-8. Rev Esp Anestesiol Reanim. 2009. PMID: 20112546 Review.
Cited by
-
Unique method for removal of knotted lumbar epidural catheter: A case report.World J Clin Cases. 2024 Apr 6;12(10):1824-1829. doi: 10.12998/wjcc.v12.i10.1824. World J Clin Cases. 2024. PMID: 38660084 Free PMC article.
-
Short-Term Outcomes of Epidural Analgesia in Minimally Invasive Esophagectomy for Esophageal Cancer: Nationwide Inpatient Data Study in Japan.Ann Surg Oncol. 2022 Dec;29(13):8225-8234. doi: 10.1245/s10434-022-12346-x. Epub 2022 Aug 12. Ann Surg Oncol. 2022. PMID: 35960454
-
[Prolonged epidural labor analgesia increases risks of epidural analgesia failure for conversion to cesarean section].Nan Fang Yi Ke Da Xue Xue Bao. 2022 Aug 20;42(8):1244-1249. doi: 10.12122/j.issn.1673-4254.2022.08.18. Nan Fang Yi Ke Da Xue Xue Bao. 2022. PMID: 36073225 Free PMC article. Chinese.
-
Ultrasound-assisted epidural labor analgesia for landmark identification in morbidly obese pregnant women: A preliminary investigation.J Clin Anesth. 2020 Feb;59:53-54. doi: 10.1016/j.jclinane.2019.05.023. Epub 2019 Jun 18. J Clin Anesth. 2020. PMID: 31226533 Free PMC article. Clinical Trial. No abstract available.
-
Increased maternal body mass index is associated with prolonged anaesthetic and surgical times for caesarean delivery but is partially offset by clinician seniority and established epidural analgesia.Aust N Z J Obstet Gynaecol. 2021 Jun;61(3):394-402. doi: 10.1111/ajo.13277. Epub 2020 Nov 28. Aust N Z J Obstet Gynaecol. 2021. PMID: 33249566 Free PMC article.
References
-
- Soens MA, Birnbach DJ, Ranasinghe JS, van Zundert A. Obstetric anesthesia for the obese and morbidly obese patient: an ounce of prevention is worth more than a pound of treatment. Acta Anaesthesiol Scand 2008;52(1):6–19. - PubMed
-
- Saravanakumar K, Rao SG, Cooper GM. Obesity and obstetric anaesthesia. Anaesthesia 2006;61(1):36–48. - PubMed
-
- Roofthooft E Anesthesia for the morbidly obese parturient. Curr Opin Anaesthesiol 2009;22(3):341–6. - PubMed
-
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity among adults: United States, 2011–2012. NCHS Data Brief 2013;(131)(131):1–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
