

The relationship between smoking intensity and subclinical cardiovascular injury: The Multi-Ethnic Study of Atherosclerosis (MESA)
- PMID: 28237909
- PMCID: PMC5404388
- DOI: 10.1016/j.atherosclerosis.2017.01.021
The relationship between smoking intensity and subclinical cardiovascular injury: The Multi-Ethnic Study of Atherosclerosis (MESA)
Abstract
Background and aims: Modern tobacco regulatory science requires an understanding of which biomarkers of cardiovascular injury are most sensitive to cigarette smoking exposure.
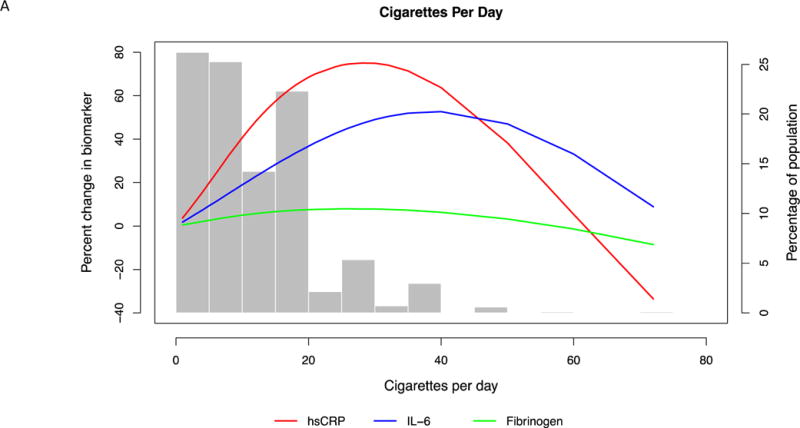
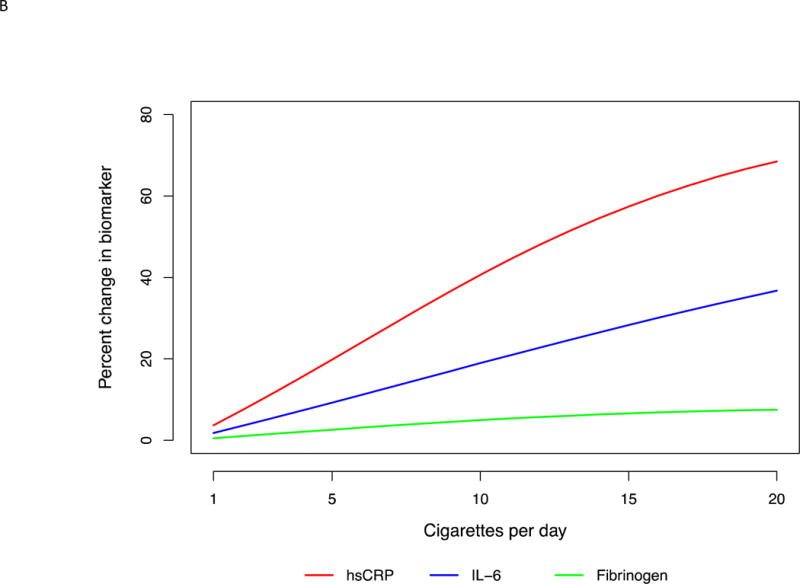
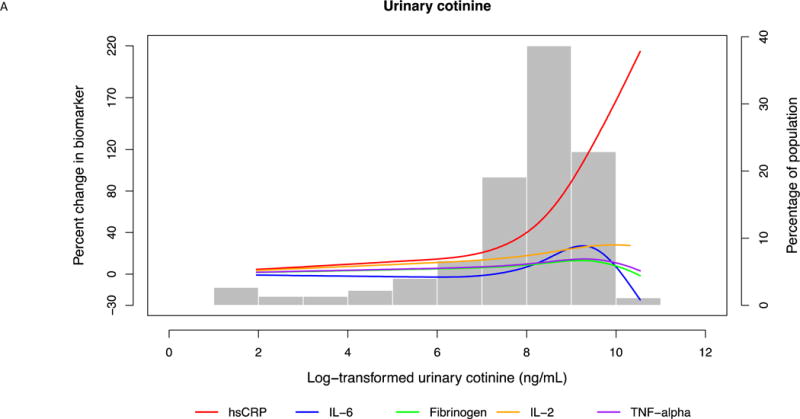
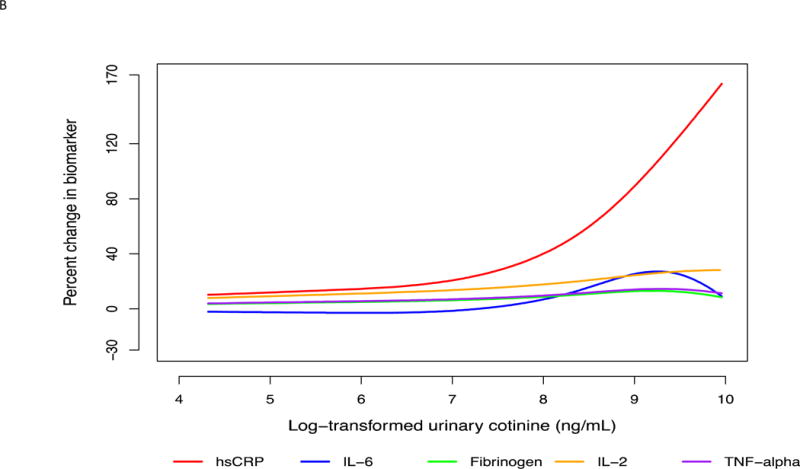
Methods: We studied self-reported current smokers from the Multi-Ethnic Study of Atherosclerosis. Smoking intensity was defined by number of cigarettes/day and urinary cotinine levels. Subclinical cardiovascular injury was assessed using markers of inflammation [high-sensitivity C-reactive protein (hsCRP), interleukin 6 & 2 (IL-2 & IL-6), tumor necrosis factor alpha (TNF-α)], thrombosis (fibrinogen, D-dimer, homocysteine), myocardial injury (troponin T; TnT), endothelial damage (albumin: creatinine ratio), and vascular function [aortic & carotid distensibility, flow-mediated dilation (FMD)]. Biomarkers were modeled as absolute and percent change using multivariable-adjusted linear regression models adjusted for cardiovascular risk factors and smoking duration.
Results: Among 843 current smokers, mean age was 58 (9) years, 53% were men, 39% were African American, mean number of cigarettes per day was 13 (10), and median smoking duration was 39 (15) years. Cigarette count was significantly associated with higher hsCRP, IL-6 and fibrinogen (β coefficients: 0.013, 0.011, 0.60 respectively), while ln-transformed cotinine was associated with the same biomarkers (β coefficients: 0.12, 0.04, 5.3 respectively) and inversely associated with aortic distensibility (β coefficient: -0.13). There was a limited association between smoking intensity and homocysteine, D-dimer, and albumin:creatinine ratio in partially adjusted models only, while there was no association with IL-2, TNF-α, carotid distensibility, FMD, or TnT in any model. In percent change analyses, relationships were strongest with hsCRP.
Conclusions: Smoking intensity was associated with early biomarkers of CVD, particularly, markers of systemic inflammation. Of these, hsCRP may be the most sensitive.
Keywords: Cigarette smoking; Endothelial damage; Inflammation; Myocardial injury; Smoking intensity; Thrombosis; Tobacco regulatory science; Vascular dysfunction.
Copyright © 2017 Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declared they do not have anything to disclose regarding no conflict of interest with respect to this manuscript.
Figures
References
-
- WHO. WHO report on the global tobacco epidemic. 2011 http://www.who.int/tobacco/global_report/2011/en/. Accessed November 14, 2015.
-
- The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. http://www-ncbi-nlm-nih-gov.ezproxy.welch.jhmi.edu/pubmed/?term=.The+Hea.... Accessed May 7, 2014.
Publication types
MeSH terms
Substances
Grants and funding
- P50 HL120163/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- U54 HL120163/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- P30 ES009089/ES/NIEHS NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
