

Two cases of resectable pancreatic cancer diagnosed by open surgical biopsy after endoscopic ultrasound fine-needle aspiration failed to yield diagnosis: case reports
- PMID: 28238191
- PMCID: PMC5326629
- DOI: 10.1186/s40792-017-0314-2
Two cases of resectable pancreatic cancer diagnosed by open surgical biopsy after endoscopic ultrasound fine-needle aspiration failed to yield diagnosis: case reports
Abstract
Background: Tumor biopsy for histological diagnosis is required preoperatively and before initiating chemotherapy or radiation therapy for patients with pancreatic cancer (Cancer of the Pancreas: Clinical Practice Guidelines, European Society for Medical Oncology). Endoscopic ultrasound fine-needle aspiration (EUS-FNA) is widely applied to obtain tissue samples for histological examination. However, in some cases, EUS-FNA cannot be performed safely or tissue samples are insufficient to establish a definitive diagnosis. We present two cases of pancreatic cancer diagnosed by open surgical biopsy after EUS-FNA failed to yield a diagnosis.
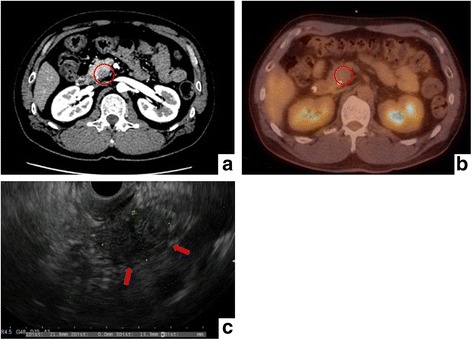
Case presentation: Case 1 was a 50-year-old man. Computed tomography showed a hypovascular lesion in the uncus of the pancreas. Although EUS-FNA was conducted twice, we could not collect enough quantity of tissue samples to establish a definitive diagnosis. Open surgical biopsy revealed adenocarcinoma, and the patient underwent preoperative chemoradiation therapy followed by curative operation. Case 2 was a 68-year-old man. Computed tomography showed a hypovascular tumor in the uncus of the pancreas. EUS revealed a 14-mm hypoechoic lesion, but we could not perform EUS-FNA because the superior mesenteric vein was located in the puncture line. Open surgical biopsy revealed adenocarcinoma, and the patient underwent preoperative chemoradiation therapy followed by pancreaticoduodenectomy.
Conclusions: EUS-FNA is the first choice in the diagnostic modalities of pancreatic neoplasm, but open surgical biopsy is an effective diagnostic method if EUS-FNA is unsuccessful.
Keywords: Intraoperative pancreas biopsy; Open surgical biopsy; Pancreatic cancer.
Figures



Similar articles
-
Needle tract seeding following endoscopic ultrasound-guided fine-needle aspiration for pancreatic cancer: a report of two cases.World J Surg Oncol. 2019 Aug 5;17(1):134. doi: 10.1186/s12957-019-1681-x. World J Surg Oncol. 2019. PMID: 31382964 Free PMC article.
-
Efficacy of endoscopic ultrasound fine needle aspiration in diagnosing the rare (non-adenocarcinoma) tumors of pancreas.Acta Gastroenterol Belg. 2014 Sep;77(3):312-7. Acta Gastroenterol Belg. 2014. PMID: 25509202
-
Pretherapeutic evaluation of patients with upper gastrointestinal tract cancer using endoscopic and laparoscopic ultrasonography.Dan Med J. 2012 Dec;59(12):B4568. Dan Med J. 2012. PMID: 23290296 Review.
-
Utility of endoscopic ultrasound-guided fine-needle aspiration in pancreatic cancer patients who failed to obtain a pathological diagnosis in surgical exploration.Gland Surg. 2022 Feb;11(2):426-431. doi: 10.21037/gs-21-913. Gland Surg. 2022. PMID: 35284304 Free PMC article.
-
Primary pancreatic leiomyosarcoma with metastasis to the liver diagnosed by endoscopic ultrasound-guided fine needle aspiration and fine needle biopsy: A Case Report and Review of Literature.Diagn Cytopathol. 2016 Dec;44(12):1070-1073. doi: 10.1002/dc.23540. Epub 2016 Jul 26. Diagn Cytopathol. 2016. PMID: 27455910 Review.
Cited by
-
Case Report: A case of occult insulinoma localized by [18F] FB (ePEG12)12-exendin-4 positron emission tomography with negative findings of selective arterial calcium stimulation test.Front Endocrinol (Lausanne). 2025 May 8;16:1556813. doi: 10.3389/fendo.2025.1556813. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40405975 Free PMC article.
References
-
- Nitta T, Nakamura T, Mitsuhashi T, Asano T, Okamura K, Tsuchikawa T, et al. The impact of margin status determined by the one-millimeter rule on tumor recurrence and survival following pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. Surg Today. 2016. doi:10.1007/s00595-016-1420-7. - PubMed
-
- Watanabe Y, Nishihara K, Matsumoto S, Okayama T, Abe Y, Nakano T. Effect of postoperative major complications on prognosis after pancreatectomy for pancreatic cancer: a retrospective review. Surg Today. 2016. doi:10.1007/s00595-016-1426-1. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
