

Suspecting non-cystic fibrosis bronchiectasis: What the busy primary care clinician needs to know
- PMID: 28238229
- PMCID: PMC5396137
- DOI: 10.1111/ijcp.12924
Suspecting non-cystic fibrosis bronchiectasis: What the busy primary care clinician needs to know
Abstract
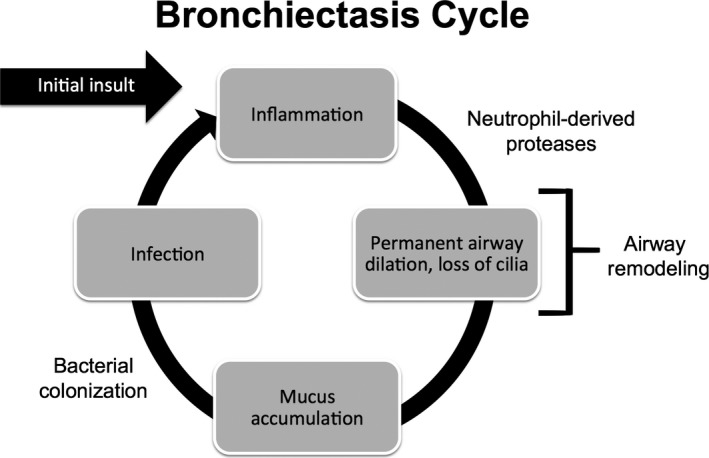
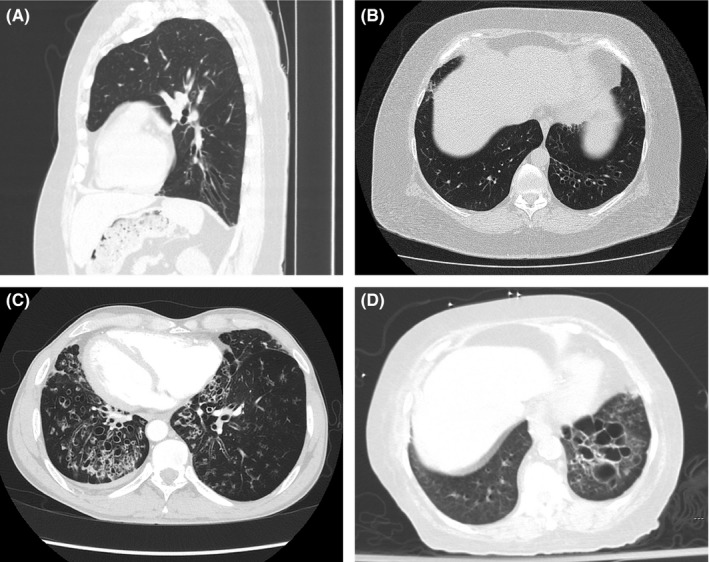
Aims: Non-cystic fibrosis bronchiectasis (NCFB) is a chronic, progressive respiratory disorder characterised by irreversibly and abnormally dilated airways, persistent cough, excessive sputum production and recurrent pulmonary infections. In the last several decades, its prevalence has increased, making it likely to be encountered in the primary care setting. The aim was to review the clinical presentation and diagnosis of NCFB, with an emphasis on the role of computed tomography (CT).
Methods: For this review, trials and reports were identified from PubMed/Medline and ClinicalTrials.gov from the US NIH and the Cochrane Register of Controlled Trials. The search used keywords: bronchiectasis, non-cystic fibrosis bronchiectasis, chronic pulmonary infection and computed tomography. No date/language restrictions were used.
Results: Non-cystic fibrosis bronchiectasis often coexists with other respiratory conditions, such as chronic obstructive pulmonary disease. The prevalence of NCFB is increasing, particularly in women and older individuals, possibly as a result of increased physician awareness and widespread use of CT, which is the gold standard for the diagnosis of NCFB. CT can assist in identifying an underlying cause of NCFB and determining the extent and severity of the disease.
Discussion: Non-cystic fibrosis bronchiectasis should be suspected in the primary care setting in patients with chronic cough, purulent sputum and frequent respiratory infections that tend to resolve slowly or partially. Early diagnosis and determination of the extent and severity of the disease by CT and other tests are critical to establish therapy to improve quality of life and potentially slow progressive decline of lung function in patients with NCFB.
© 2016 The Authors. Haemophilia published by John Wiley & Sons Ltd.
Figures

Similar articles
-
Assessing effects of inhaled antibiotics in adults with non-cystic fibrosis bronchiectasis--experiences from recent clinical trials.Expert Rev Respir Med. 2018 Sep;12(9):769-782. doi: 10.1080/17476348.2018.1503540. Epub 2018 Aug 3. Expert Rev Respir Med. 2018. PMID: 30025482 Review.
-
Management of Non-Cystic Fibrosis Bronchiectasis.Consult Pharm. 2018 Nov 1;33(11):658-666. doi: 10.4140/TCP.n.2018.658.. Consult Pharm. 2018. PMID: 30458908
-
Inhaled antibiotics therapy for stable non-cystic fibrosis bronchiectasis: a meta-analysis.Ther Adv Respir Dis. 2020 Jan-Dec;14:1753466620936866. doi: 10.1177/1753466620936866. Ther Adv Respir Dis. 2020. PMID: 32615859 Free PMC article.
-
Effect of macrolide on lung function and computed tomography (CT) score in non-cystic fibrosis bronchiectasis.Acta Clin Belg. 2012 Sep-Oct;67(5):338-46. doi: 10.2143/ACB.67.5.2062687. Acta Clin Belg. 2012. PMID: 23189541
-
Spotlight on inhaled ciprofloxacin and its potential in the treatment of non-cystic fibrosis bronchiectasis.Drug Des Devel Ther. 2018 Nov 27;12:4059-4066. doi: 10.2147/DDDT.S168014. eCollection 2018. Drug Des Devel Ther. 2018. PMID: 30568427 Free PMC article. Review.
Cited by
-
Epithelial-Mesenchymal Transition Mechanisms in Chronic Airway Diseases: A Common Process to Target?Int J Mol Sci. 2023 Aug 3;24(15):12412. doi: 10.3390/ijms241512412. Int J Mol Sci. 2023. PMID: 37569787 Free PMC article. Review.
-
Health care experiences of mothers of children with bronchiectasis in Counties Manukau, Auckland, New Zealand.BMC Health Serv Res. 2018 Sep 19;18(1):722. doi: 10.1186/s12913-018-3532-9. BMC Health Serv Res. 2018. PMID: 30231872 Free PMC article.
-
Biofilm Formations in Pediatric Respiratory Tract Infection : Part 1: Biofilm Structure, Role of Innate Immunity in Protection Against and Response to Biofilm, Methods of Biofilm Detection, Pediatric Respiratory Tract Diseases Associated with Mucosal Biofilm Formation.Curr Infect Dis Rep. 2019 Feb 28;21(2):6. doi: 10.1007/s11908-019-0658-9. Curr Infect Dis Rep. 2019. PMID: 30820766 Review.
-
Small Airway Disease and Emphysema Are Associated with Future Exacerbations in Smokers with CT-derived Bronchiectasis and COPD: Results from the COPDGene Cohort.Radiology. 2021 Sep;300(3):706-714. doi: 10.1148/radiol.2021204052. Epub 2021 Jun 22. Radiology. 2021. PMID: 34156303 Free PMC article.
-
Evaluating elexacaftor/tezacaftor/ivacaftor (ETI; Trikafta™) for treatment of patients with non-cystic fibrosis bronchiectasis (NCFBE): A clinical study protocol.PLoS One. 2025 Feb 14;20(2):e0316721. doi: 10.1371/journal.pone.0316721. eCollection 2025. PLoS One. 2025. PMID: 39951444 Free PMC article.
References
-
- Pasteur MC, Bilton D, Hill AT; on behalf of the British Thoracic Society Bronchiectasis (non‐CF) Guideline Group . British Thoracic Society guideline for non‐CF bronchiectasis. Thorax. 2010; 65 (Suppl. 1): i1–i58. - PubMed
-
- Goeminne P, Dupont L. Non‐cystic fibrosis bronchiectasis: diagnosis and management in 21st century. Postgrad Med J. 2010;86:493–501. - PubMed
-
- Altenburg J, Wortel K, van der Werf TS, Boersma WG. Non‐cystic fibrosis bronchiectasis: clinical presentation, diagnosis and treatment, illustrated by data from a Dutch Teaching Hospital. Neth J Med. 2015;73:147–154. - PubMed
-
- Weycker D, Edelsberg J, Oster G, Tino G. Prevalence and economic burden of bronchiectasis. Clin Pulm Med. 2005;12:205–209.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical