

[Irritable bowel syndrome with constipation and functional constipation in adults: Treatment (Part 2 of 2)]
- PMID: 28238460
- PMCID: PMC6875999
- DOI: 10.1016/j.aprim.2017.01.003
[Irritable bowel syndrome with constipation and functional constipation in adults: Treatment (Part 2 of 2)]
Abstract
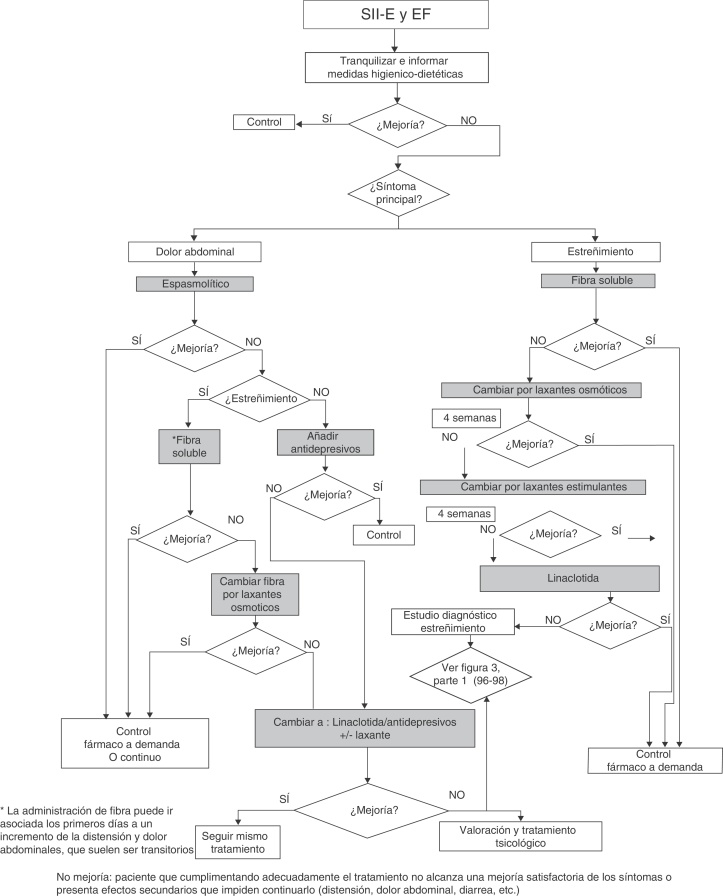
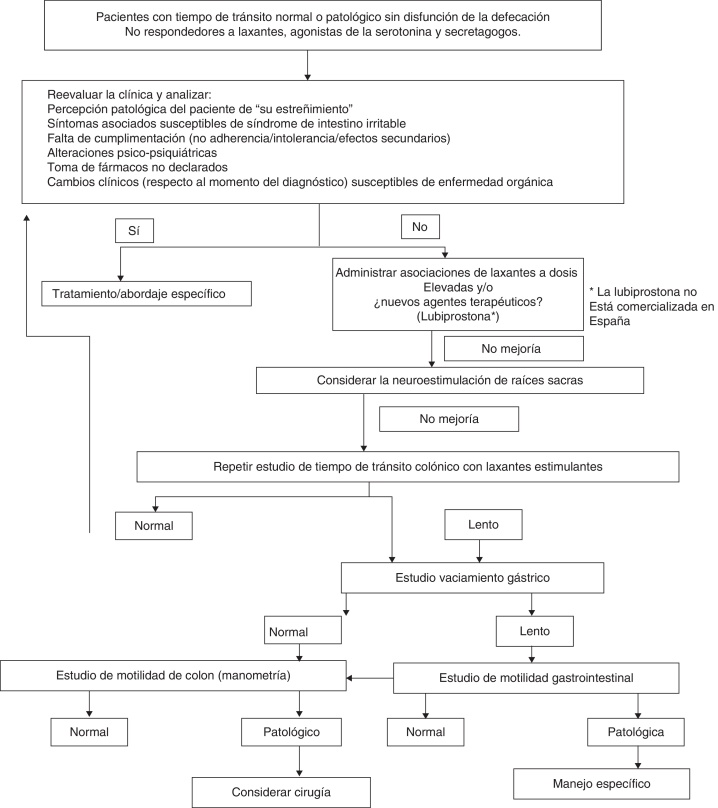
In this Clinical practice guide we examine the diagnostic and therapeutic management of adult patients with constipation and abdominal discomfort, at the confluence of the spectrum of irritable bowel syndrome and functional constipation. Both fall within the framework of functional intestinal disorders and have major personal, health and social impact, altering the quality of life of the patients affected. The former is a subtype of irritable bowel syndrome in which constipation and altered bowel habit predominate, often along with recurring abdominal pain, bloating and abdominal distension. Constipation is characterised by infrequent or hard-to-pass bowel movements, often accompanied by straining during defecation or the sensation of incomplete evacuation. There is no underlying organic cause in the majority of cases; it being considered a functional bowel disorder. There are many clinical and pathophysiological similarities between the two conditions, the constipation responds in a similar way to commonly used drugs, the fundamental difference being the presence or absence of pain, but not in an "all or nothing" way. The severity of these disorders depends not only on the intensity of the intestinal symptoms but also on other biopsychosocial factors: association of gastrointestinal and extraintestinal symptoms, degree of involvement, forms of perception and behaviour. Functional bowel disorders are diagnosed using the Rome criteria. This Clinical practice guide adapts to the Rome IV criteria published at the end of May 2016. The first part (96, 97, 98) examined the conceptual and pathophysiological aspects, alarm criteria, diagnostic test and referral criteria between Primary Care and Gastroenterology. This second part reviews all the available treatment alternatives (exercise, fluid ingestion, diet with soluble fibre-rich foods, fibre supplements, other dietary components, osmotic or stimulating laxatives, probiotics, antibiotics, spasmolytics, peppermint essence, prucalopride, linaclotide, lubiprostone, biofeedback, antdepressants, psychological treatment, acupuncture, enemas, sacral root neurostimulation and surgery), and practical recommendations are made for each.
En esta Guía de práctica clínica analizamos el manejo diagnóstico y terapéutico de pacientes adultos con estreñimiento y molestias abdominales, bajo la confluencia del espectro del síndrome del intestino irritable y el estreñimiento funcional. Ambas patologías están encuadradas en los trastornos funcionales intestinales y tienen una importante repercusión personal, sanitaria y social, afectando a la calidad de vida de los pacientes que las padecen. La primera es el subtipo de síndrome del intestino irritable en el que el estreñimiento es la alteración deposicional predominante junto con dolor abdominal recurrente, hinchazón y distensión abdominal frecuente. El estreñimiento se caracteriza por la dificultad o la escasa frecuencia en relación con las deposiciones, a menudo acompañado por esfuerzo excesivo durante la defecación o sensación de evacuación incompleta. En la mayoría de los casos no tiene una causa orgánica subyacente, siendo considerado un trastorno funcional intestinal. Son muchas las similitudes clínicas y fisiopatológicas entre ambos trastornos, con respuesta similar del estreñimiento a fármacos comunes, siendo la diferencia fundamental la presencia o ausencia de dolor, pero no de un modo evaluable como «todo o nada». La gravedad de estos trastornos depende no solo de la intensidad de los síntomas intestinales sino también de otros factores biopsicosociales: asociación de síntomas gastrointestinales y extraintestinales, grado de afectación, y formas de percepción y comportamiento. Mediante los criterios de Roma, se diagnostican los trastornos funcionales intestinales. Esta Guía de práctica clínica está adaptada a los criterios de Roma
Keywords: Abdominal discomfort; Adultos; Adults; Atención Primaria; Clinical practice guide; Digestive diseases; Enfermedades digestivas; Estreñimiento funcional; Functional constipation; Guía de práctica clínica; Irritable bowel syndrome; Molestia abdominal; Primary care; Roma IV; Rome IV; Síndrome del intestino irritable.
Copyright © 2017 Elsevier España, S.L.U. All rights reserved.
Figures
Similar articles
-
[Irritable bowel syndrome with constipation and functional constipation in adults: Treatment (Part 2 of 2)].Semergen. 2017 Mar;43(2):123-140. doi: 10.1016/j.semerg.2017.01.001. Epub 2017 Feb 8. Semergen. 2017. PMID: 28189496 Spanish.
-
[Clinical practice guidelines: Irritable bowel syndrome with constipation and functional constipation in adults: Concept, diagnosis, and healthcare continuity. (Part 1 of 2)].Aten Primaria. 2017 Jan;49(1):42-55. doi: 10.1016/j.aprim.2016.11.003. Epub 2016 Dec 24. Aten Primaria. 2017. PMID: 28027792 Free PMC article. Spanish.
-
[Clinical practice guidelines: Irritable bowel syndrome with constipation and functional constipation in adults: Concept, diagnosis, and healthcare continuity. (Part 1 of 2)].Semergen. 2017 Jan-Feb;43(1):43-56. doi: 10.1016/j.semerg.2016.06.009. Epub 2016 Oct 31. Semergen. 2017. PMID: 27810257 Spanish.
-
Clinical Practice Guideline: Irritable bowel syndrome with constipation and functional constipation in the adult.Rev Esp Enferm Dig. 2016 Jun;108(6):332-63. doi: 10.17235/reed.2016.4389/2016. Rev Esp Enferm Dig. 2016. PMID: 27230827 Review.
-
The use of novel promotility and prosecretory agents for the treatment of chronic idiopathic constipation and irritable bowel syndrome with constipation.Adv Ther. 2009 May;26(5):519-30. doi: 10.1007/s12325-009-0027-4. Epub 2009 May 14. Adv Ther. 2009. PMID: 19444393 Review.
Cited by
-
Acupoint Massage Therapy Alters the Composition of Gut Microbiome in Functional Constipation Patients.Evid Based Complement Alternat Med. 2021 Jan 12;2021:1416236. doi: 10.1155/2021/1416236. eCollection 2021. Evid Based Complement Alternat Med. 2021. PMID: 33505487 Free PMC article.
-
Supplementation with probiotics, prebiotics, and synbiotics in patients with chronic functional constipation: a randomized, double-blind, placebo-controlled pilot clinical trial.Gastroenterol Rep (Oxf). 2024 Nov 11;12:goae101. doi: 10.1093/gastro/goae101. eCollection 2024. Gastroenterol Rep (Oxf). 2024. PMID: 39530075 Free PMC article.
-
Observation of the Intervention Effect of Biofeedback Therapy Combined With Cluster Nursing on Perioperative Constipation in Patients With Thoracolumbar Fracture.Front Surg. 2022 Mar 7;9:847068. doi: 10.3389/fsurg.2022.847068. eCollection 2022. Front Surg. 2022. PMID: 35321074 Free PMC article.
References
-
- Mearin F., Ciriza C., Minguez M., Rey E., Mascort J.J., Pena E. Clinical Practice Guideline: Irritable bowel syndrome with constipation and functional constipation in the adult. Rev Esp Enferm Dig. 2016;108:332–363. - PubMed
-
- Lacy B.E., Mearin F., Chang L., Chey W.D., Lembo A.J., Simren M. Bowel disorders. Gastroenterology. 2016;150:1393–1407. - PubMed
-
- De Schryver A.M., Keulemans Y.C., Peters H.P., Akkermans L.M., Smout A.J., De Vries W.R. Effects of regular physical activity on defecation pattern in middle-aged patients complaining of chronic constipation. Scand J Gastroenterol. 2005;40:422–429. PMID: 16028436. - PubMed
-
- Villoria A., Serra J., Azpiroz F., Malagelada J.-R. Physical activity and intestinal gas clearance in patients with bloating. Am J Gastroenterol. 2006;101:2552–2557. PMID: 17029608. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
