

Out-of-Hospital Triage of Older Adults With Head Injury: A Retrospective Study of the Effect of Adding "Anticoagulation or Antiplatelet Medication Use" as a Criterion
- PMID: 28238499
- PMCID: PMC5522761
- DOI: 10.1016/j.annemergmed.2016.12.018
Out-of-Hospital Triage of Older Adults With Head Injury: A Retrospective Study of the Effect of Adding "Anticoagulation or Antiplatelet Medication Use" as a Criterion
Abstract
Study objective: Field triage guidelines recommend that emergency medical services (EMS) providers consider transport of head-injured older adults with anticoagulation use to trauma centers. However, the triage patterns and the incidence of intracranial hemorrhage or neurosurgery in these patients are unknown. Our objective is to describe the characteristics and outcomes of older adults with head trauma who are transported by EMS, particularly for patients who do not meet physiologic, anatomic, or mechanism-of-injury (steps 1 to 3) field triage criteria but are receiving anticoagulant or antiplatelet medications.
Methods: This was a retrospective study at 5 EMS agencies and 11 hospitals (4 trauma centers, 7 nontrauma centers). Patients aged 55 years or older with head trauma who were transported by EMS were included. The primary outcome was the presence of intracranial hemorrhage. The secondary outcome was a composite measure of inhospital death or neurosurgery.
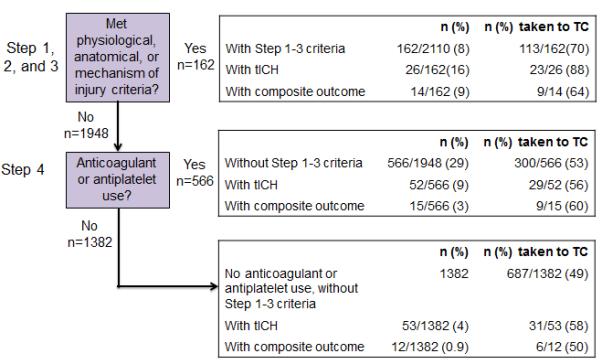
Results: Of the 2,110 patients included, 131 (6%) had intracranial hemorrhage and 41 (2%) had inhospital death or neurosurgery. There were 162 patients (8%) with steps 1 to 3 criteria. Of the remaining 1,948 patients without steps 1 to 3 criteria, 566 (29%) had anticoagulant or antiplatelet use. Of these patients, 52 (9%) had traumatic intracranial hemorrhage and 15 (3%) died or had neurosurgery. The sensitivity (adjusted for clustering by EMS agency) of steps 1 to 3 criteria was 19.8% (26/131; 95% confidence interval [CI] 5.5% to 51.2%) for identifying traumatic intracranial hemorrhage and 34.1% (14/41; 95% CI 9.9% to 70.1%) for death or neurosurgery. The additional criterion of anticoagulant or antiplatelet use improved the sensitivity for intracranial hemorrhage (78/131; 59.5%; 95% CI 42.9% to 74.2%) and death or neurosurgery (29/41; 70.7%; 95% CI 61.0% to 78.9%).
Conclusion: Relatively few patients met steps 1 to 3 triage criteria. For individuals who did not have steps 1 to 3 criteria, nearly 30% had anticoagulant or antiplatelet use. A relatively high proportion of these patients had intracranial hemorrhage, but a much smaller proportion died or had neurosurgery during hospitalization. Use of steps 1 to 3 triage criteria alone is not sufficient in identifying intracranial hemorrhage and death or neurosurgery in this patient population. The additional criterion of anticoagulant or antiplatelet use improves the sensitivity of the instrument, with only a modest decrease in specificity.
Copyright © 2016 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Can an Out-of-Hospital Medication History Save Lives for Injured Older Adults?Ann Emerg Med. 2017 Aug;70(2):139-141. doi: 10.1016/j.annemergmed.2017.02.005. Epub 2017 Mar 28. Ann Emerg Med. 2017. PMID: 28363397 No abstract available.
References
-
- Faul MXL, Wal MM, Coronado VG. Traumatic brain injury in the United States: emergency department visits, hospitalizations, and deaths 2002-2006. US Department of Health and Human Services, CDC; Atlanta, GA: 2010.
-
- Ma VY, Chan L, Carruthers KJ. Incidence, prevalence, costs, and impact on disability of common conditions requiring rehabilitation in the United States: stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, osteoarthritis, rheumatoid arthritis, limb loss, and back pain. Arch Phys Med Rehabil. 2014;95(5):986–995. - PMC - PubMed
-
- McMillian WD, Rogers FB. Management of prehospital antiplatelet and anticoagulant therapy in traumatic head injury: a review. J Trauma. 2009;66(3):942–950. - PubMed
-
- Rathlev NK, Medzon R, Lowery D, et al. Intracranial pathology in elders with blunt head trauma. Acad Emerg Med. 2006;13(3):302–307. - PubMed
-
- Mushkudiani NA, Engel DC, Steyerberg EW, et al. Prognostic value of demographic characteristics in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24(2):259–269. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
