

Effect of angina under-recognition on treatment in outpatients with stable ischaemic heart disease
- PMID: 28239488
- PMCID: PMC5322471
- DOI: 10.1093/ehjqcco/qcw016
Effect of angina under-recognition on treatment in outpatients with stable ischaemic heart disease
Abstract
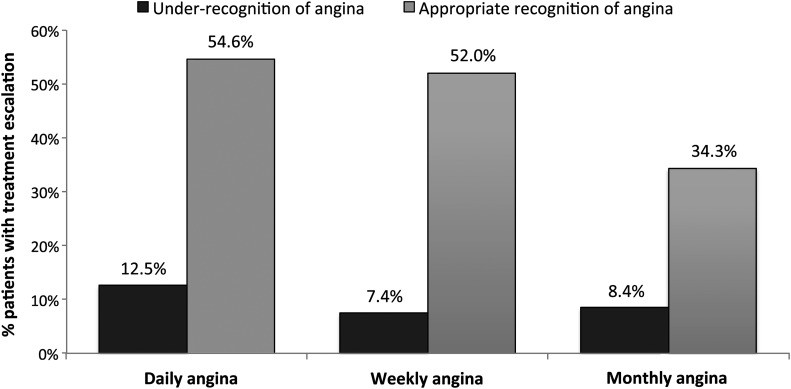
Aims: Almost a third of outpatients with chronic coronary artery disease (CAD) report having angina in the prior month, which is frequently under-recognized by their cardiologists. Whether under-recognition is associated with less treatment escalation to control angina, and potential underuse of treatment, is unknown.
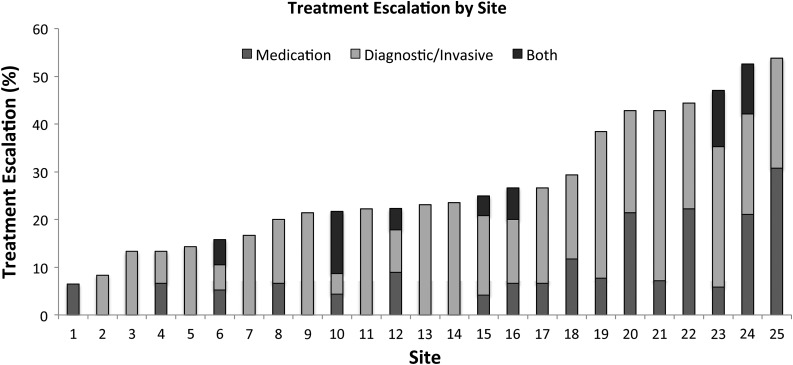
Methods and results: Patients with CAD from 25 US cardiology outpatient practices completed the Seattle Angina Questionnaire (SAQ) prior to their clinic visit, and angina was categorized as daily, weekly, monthly and no angina. Cardiologists (n=155) independently quantified patients' angina, blinded to patients' SAQ scores. Under-recognition was defined as the physician reporting a lower category of angina frequency than the patient. Among 1257 patients with CAD, 411 reported angina in the past month, of whom 178 (43.3%) patients were under-recognized. Treatment escalation-defined as intensification (up-titration or addition) of antianginal medications, referral for diagnostic testing or revascularization, or hospital admission-occurred in 106 (25.8%) patients with angina. Patients with under-recognized angina were less likely to get treatment escalation than patients whose angina was appropriately recognized (8.4% vs 39.1%, P<0.001). In a hierarchical multivariable logistic regression model adjusting for demographic and clinical characteristics, as well as the burden of angina, under-recognition remained strongly associated with a lack of treatment escalation (adjusted OR 0.10, 95% CI 0.04-0.21, P<0.001).
Conclusions: Under-recognition of angina in cardiology outpatient practices is associated with less aggressive treatment escalation and may lead to poorer angina control. Standardizing clinical recognition of angina using validated tools could reduce under-recognition of angina, facilitate treatment, and potentially improve outcomes.
Keywords: angina; antianginal medications; coronary artery disease; quality of care.
Conflict of interest statement
Disclosure of potential conflicts of interest. The remaining authors have no relevant relationships to disclose.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB, American Heart Association Statistics C, Stroke Statistics S. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation 2015;131:e29–e322. - PubMed
-
- Weintraub WS, Spertus JA, Kolm P, Maron DJ, Zhang Z, Jurkovitz C, Zhang W, Hartigan PM, Lewis C, Veledar E, Bowen J, Dunbar SB, Deaton C, Kaufman S, O'Rourke RA, Goeree R, Barnett PG, Teo KK, Boden WE, Group CTR, Mancini GB. Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med 2008;359:677–687. - PubMed
-
- Fihn SD, Gardin JM, Abrams J, Berra K, Blankenship JC, Dallas AP, Douglas PS, Foody JM, Gerber TC, Hinderliter AL, King SB 3rd, Kligfield PD, Krumholz HM, Kwong RY, Lim MJ, Linderbaum JA, Mack MJ, Munger MA, Prager RL, Sabik JF, Shaw LJ, Sikkema JD, Smith CR Jr, Smith SC Jr, Spertus JA, Williams SV, American College of Cardiology F, American Heart Association Task Force on Practice G, American College of P, American Association for Thoracic S, Preventive Cardiovascular Nurses A, Society for Cardiovascular A, Interventions, Society of Thoracic S. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2012;60:e44–e164. - PubMed
-
- Kernis SJ, Harjai KJ, Stone GW, Grines LL, Boura JA, O'Neill WW, Grines CL. Does beta-blocker therapy improve clinical outcomes of acute myocardial infarction after successful primary angioplasty? J Am Coll Cardiol 2004;43:1773–1779. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
