

Measures of metabolism and complexity in the brain of patients with disorders of consciousness
- PMID: 28239544
- PMCID: PMC5318348
- DOI: 10.1016/j.nicl.2017.02.002
Measures of metabolism and complexity in the brain of patients with disorders of consciousness
Abstract
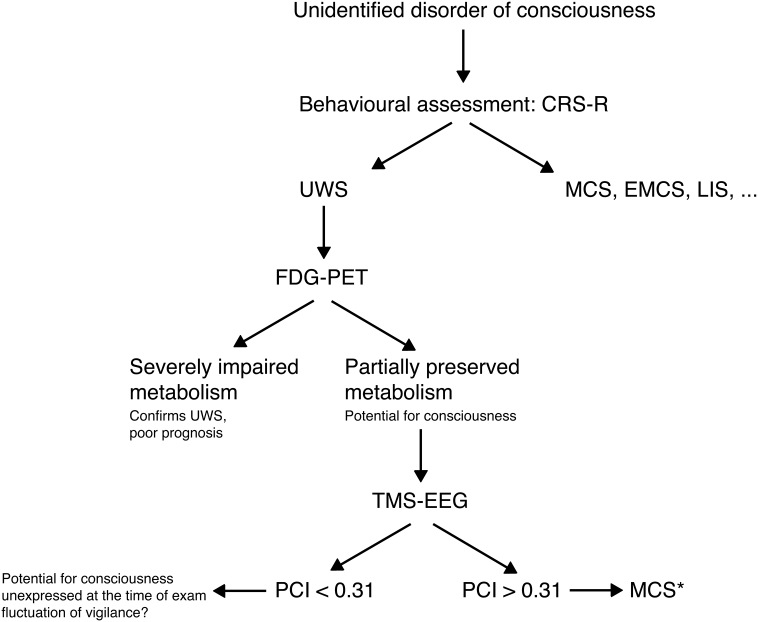
Background: Making an accurate diagnosis in patients with disorders of consciousness remains challenging. 18F-fluorodeoxyglucose (FDG)-PET has been validated as a diagnostic tool in this population, and allows identifying unresponsive patients with a capacity for consciousness. In parallel, the perturbational complexity index (PCI), a new measure based on the analysis of the electroencephalographic response to transcranial magnetic stimulation, has also been suggested as a tool to distinguish between unconscious and conscious states. The aim of the study was to cross-validate FDG-PET and PCI, and to identify signs of consciousness in otherwise unresponsive patients.
Methods: We jointly applied the Coma Recovery Scale-Revised, FDG-PET and PCI to assess 24 patients with non-acute disorders of consciousness or locked-in syndrome (13 male; 19-54 years old; 12 traumatic; 9 unresponsive wakefulness syndrome, 11 minimally conscious state; 2 emergence from the minimally conscious state, and 2 locked-in syndrome).
Results: FDG-PET and PCI provided congruent results in 22 patients, regardless of their behavioural diagnosis. Notably, FDG-PET and PCI revealed preserved metabolic rates and high complexity levels in four patients who were behaviourally unresponsive.
Conclusion: We propose that jointly measuring the metabolic activity and the electrophysiological complexity of cortical circuits is a useful complement to the diagnosis and stratification of patients with disorders of consciousness.
Keywords: Brain injury; CRS-R, Coma Recovery Scale-Revised; DOC, disorders of consciousness; Disorders of consciousness; EMCS, emergence from the minimally conscious state; Electroencephalography; FDG, 18F-fluorodeoxyglucose; LIS, locked-in syndrome; MCS*, non-behavioural minimally conscious state; MCS, minimally conscious state; PCI, perturbational complexity index; Positron emission tomography; SPM, statistical parametric mapping; TMS–EEG, transcranial magnetic stimulation coupled with high-density EEG; Transcranial magnetic stimulation; UWS, unresponsive wakefulness syndrome; Unresponsive wakefulness syndrome minimally conscious state; fMRI, functional MRI.
Figures
Similar articles
-
Diagnostic precision of PET imaging and functional MRI in disorders of consciousness: a clinical validation study.Lancet. 2014 Aug 9;384(9942):514-22. doi: 10.1016/S0140-6736(14)60042-8. Epub 2014 Apr 15. Lancet. 2014. PMID: 24746174
-
Intrinsic functional connectivity differentiates minimally conscious from unresponsive patients.Brain. 2015 Sep;138(Pt 9):2619-31. doi: 10.1093/brain/awv169. Epub 2015 Jun 27. Brain. 2015. PMID: 26117367
-
Neural correlates of consciousness in patients who have emerged from a minimally conscious state: a cross-sectional multimodal imaging study.Lancet Neurol. 2016 Jul;15(8):830-842. doi: 10.1016/S1474-4422(16)00111-3. Epub 2016 Apr 27. Lancet Neurol. 2016. PMID: 27131917
-
Transcranial magnetic stimulation combined with high-density EEG in altered states of consciousness.Brain Inj. 2014;28(9):1180-9. doi: 10.3109/02699052.2014.920524. Brain Inj. 2014. PMID: 25099022 Review.
-
Assessing consciousness in coma and related states using transcranial magnetic stimulation combined with electroencephalography.Ann Fr Anesth Reanim. 2014 Feb;33(2):65-71. doi: 10.1016/j.annfar.2013.11.002. Epub 2014 Jan 6. Ann Fr Anesth Reanim. 2014. PMID: 24393302 Review.
Cited by
-
Network Mapping of Connectivity Alterations in Disorder of Consciousness: Towards Targeted Neuromodulation.J Clin Med. 2020 Mar 18;9(3):828. doi: 10.3390/jcm9030828. J Clin Med. 2020. PMID: 32197485 Free PMC article.
-
Reduced emergent character of neural dynamics in patients with a disrupted connectome.Neuroimage. 2023 Apr 1;269:119926. doi: 10.1016/j.neuroimage.2023.119926. Epub 2023 Feb 3. Neuroimage. 2023. PMID: 36740030 Free PMC article.
-
Cerebral Metabolic Changes During Sleep.Curr Neurol Neurosci Rep. 2018 Jul 16;18(9):57. doi: 10.1007/s11910-018-0868-9. Curr Neurol Neurosci Rep. 2018. PMID: 30014344 Free PMC article. Review.
-
Perturbational complexity index in assessing responsiveness to rTMS treatment in patients with disorders of consciousness: a cross-over randomized controlled trial study.J Neuroeng Rehabil. 2024 Sep 19;21(1):167. doi: 10.1186/s12984-024-01455-1. J Neuroeng Rehabil. 2024. PMID: 39300529 Free PMC article. Clinical Trial.
-
Brain state identification and neuromodulation to promote recovery of consciousness.Brain Commun. 2024 Oct 11;6(5):fcae362. doi: 10.1093/braincomms/fcae362. eCollection 2024. Brain Commun. 2024. PMID: 39474045 Free PMC article. Review.
References
-
- Bodart O., Laureys S., Gosseries O. Coma and disorders of consciousness: scientific advances and practical considerations for clinicians. Semin. Neurol. 2013;33:83–90. - PubMed
-
- Casali A.G., Gosseries O., Rosanova M., Boly M., Sarasso S., Casali K.R., Casarotto S., Bruno M.-A., Laureys S., Tononi G., Massimini M. A theoretically based index of consciousness independent of sensory processing and behavior. Sci. Transl. Med. 2013;5:1–10. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
