

Carbamazepine versus phenytoin monotherapy for epilepsy: an individual participant data review
- PMID: 28240353
- PMCID: PMC6464554
- DOI: 10.1002/14651858.CD001911.pub3
Carbamazepine versus phenytoin monotherapy for epilepsy: an individual participant data review
Update in
-
Carbamazepine versus phenytoin monotherapy for epilepsy: an individual participant data review.Cochrane Database Syst Rev. 2019 Jul 18;7(7):CD001911. doi: 10.1002/14651858.CD001911.pub4. Cochrane Database Syst Rev. 2019. PMID: 31318037 Free PMC article.
Abstract
Background: This is an updated version of the original Cochrane Review published in Issue 2, 2002 and its subsequent updates in 2010 and 2015.Epilepsy is a common neurological condition in which recurrent, unprovoked seizures are caused by abnormal electrical discharges from the brain. It is believed that with effective drug treatment, up to 70% of individuals with active epilepsy have the potential to become seizure-free and go into long-term remission shortly after starting drug therapy with a single antiepileptic drug in monotherapy.Worldwide, carbamazepine and phenytoin are commonly-used broad spectrum antiepileptic drugs, suitable for most epileptic seizure types. Carbamazepine is a current first-line treatment for partial onset seizures in the USA and Europe. Phenytoin is no longer considered a first-line treatment due to concerns over adverse events associated with its use, but the drug is still commonly used in low- to middle-income countries because of its low cost. No consistent differences in efficacy have been found between carbamazepine and phenytoin in individual trials, although the confidence intervals generated by these studies are wide. Differences in efficacy may therefore be shown by synthesising the data of the individual trials.
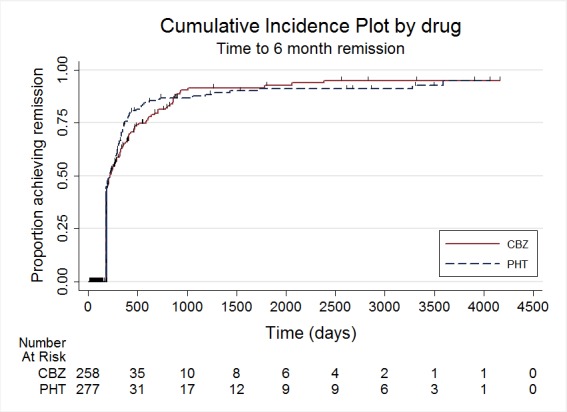
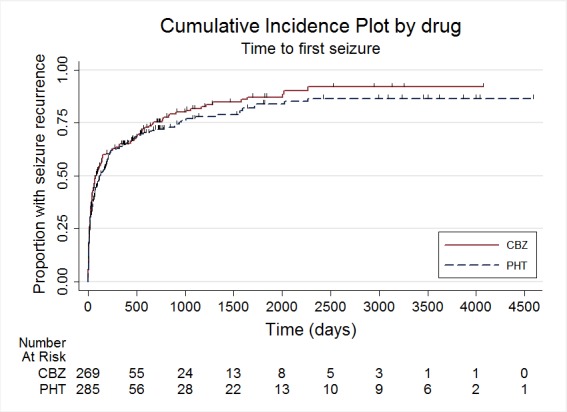
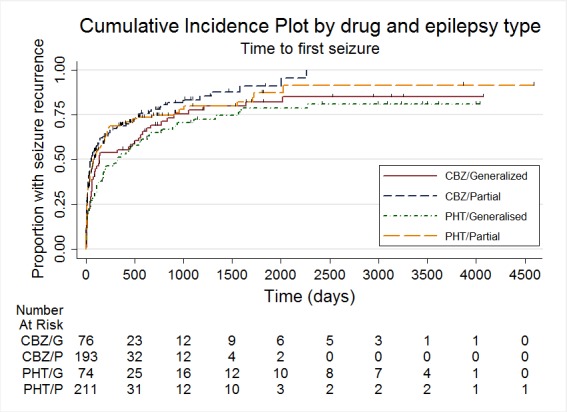
Objectives: To review the time to withdrawal, six- and 12-month remission, and first seizure with carbamazepine compared to phenytoin, used as monotherapy in people with partial onset seizures (simple partial, complex partial, or secondarily generalised tonic-clonic seizures), or generalised tonic-clonic seizures, with or without other generalised seizure types.
Search methods: For the latest update we searched the Cochrane Epilepsy Group's Specialised Register (1st November 2016), the Cochrane Central Register of Controlled Trials (CENTRAL) via the Cochrane Register of Studies Online (CRSO, 1st November 2016), MEDLINE (Ovid, 1946 to 1 November 2016), ClinicalTrials.gov (1 November 2016), and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP, 1st November 2016). Previously we also searched SCOPUS (1823 to 16th September 2014) as an alternative to Embase, but this is no longer necessary, because randomised and quasi-randomised controlled trials in Embase are now included in CENTRAL. We handsearched relevant journals, contacted pharmaceutical companies, original trial investigators and experts in the field.
Selection criteria: Randomised controlled trials (RCTs) in children or adults with partial onset seizures or generalised onset tonic-clonic seizures, comparing carbamazepine monotherapy versus phenytoin monotherapy.
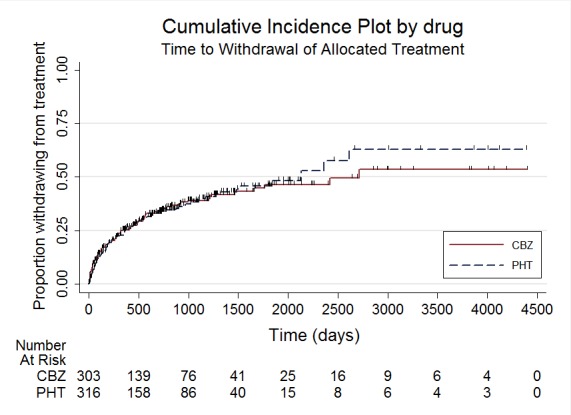
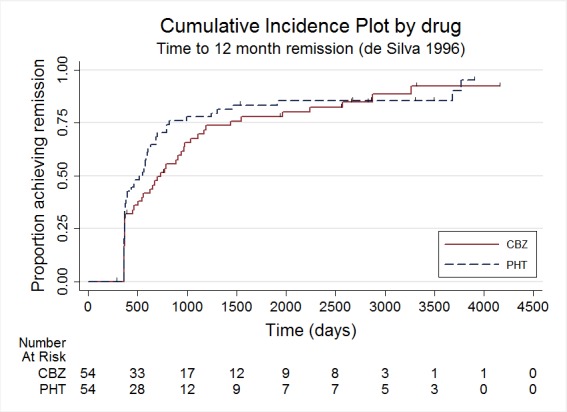
Data collection and analysis: This is an individual participant data (IPD) review. Our primary outcome was time to withdrawal of allocated treatment, and our secondary outcomes were time to six-month remission, time to 12-month remission, and time to first seizure post-randomisation. We used Cox proportional hazards regression models to obtain study-specific estimates of hazard ratios (HRs) with 95% confidence intervals (CIs) and the generic inverse variance method to obtain the overall pooled HR and 95% CI.
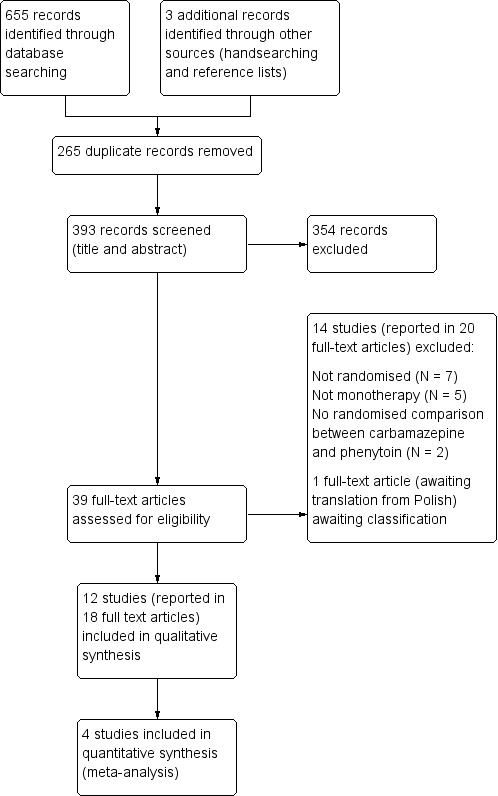
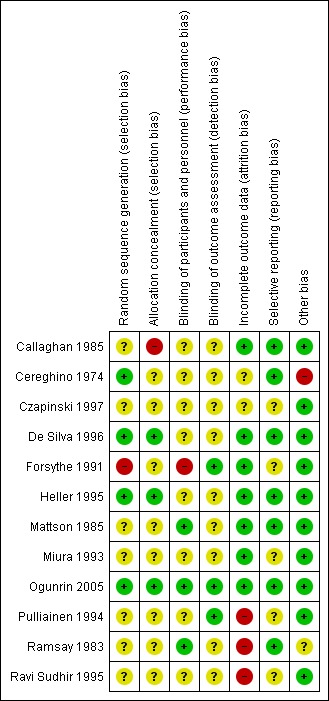
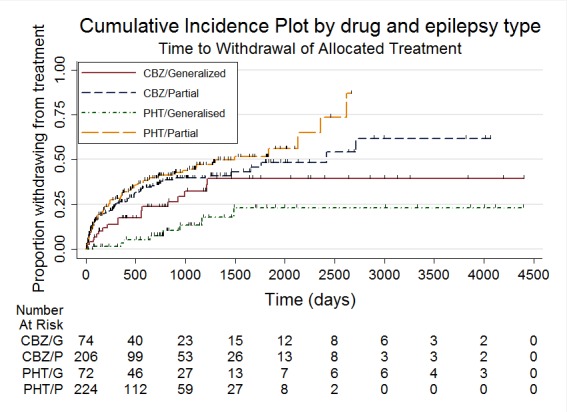
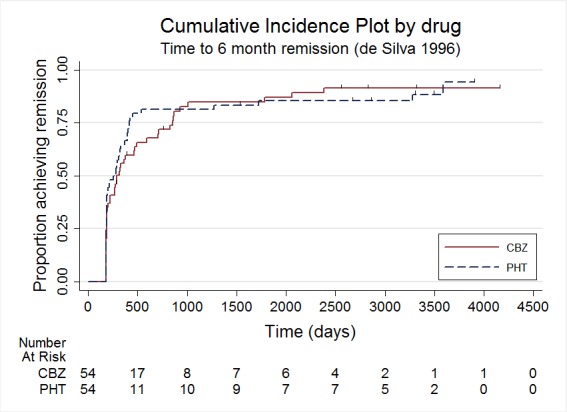
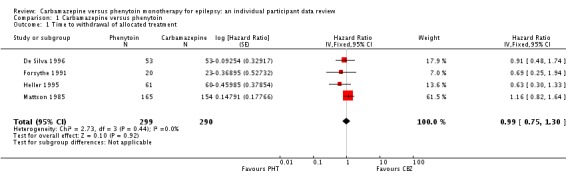
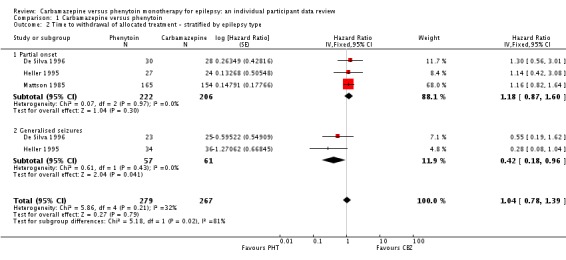
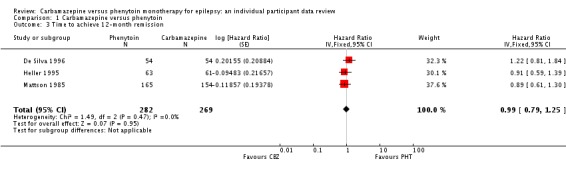
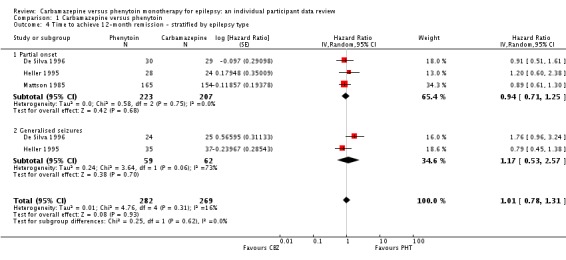
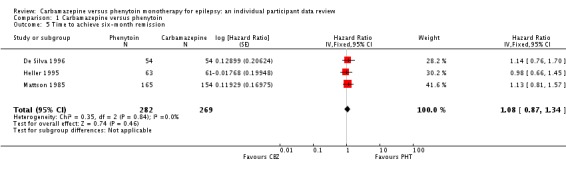
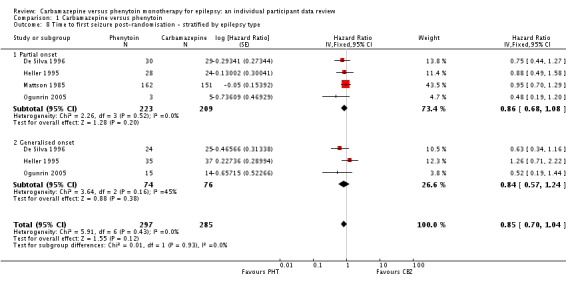
Main results: IPD were available for 595 participants out of 1192 eligible individuals, from four out of 12 trials (i.e. 50% of the potential data). For remission outcomes, HR greater than 1 indicates an advantage for phenytoin; and for first seizure and withdrawal outcomes, HR greater than 1 indicates an advantage for carbamazepine. The methodological quality of the four studies providing IPD was generally good and we rated it at low risk of bias overall in the analyses.The main overall results (pooled HR adjusted for seizure type) were time to withdrawal of allocated treatment: 1.04 (95% CI 0.78 to 1.39; three trials, 546 participants); time to 12-month remission: 1.01 (95% CI 0.78 to 1.31; three trials, 551 participants); time to six-month remission: 1.11 (95% CI 0.89 to 1.37; three trials, 551 participants); and time to first seizure: 0.85 (95% CI 0.70 to 1.04; four trials, 582 participants). The results suggest no overall statistically significant difference between the drugs for these outcomes. There is some evidence of an advantage for phenytoin for individuals with generalised onset seizures for our primary outcome (time to withdrawal of allocated treatment): pooled HR 0.42 (95% CI 0.18 to 0.96; two trials, 118 participants); and a statistical interaction between treatment effect and epilepsy type (partial versus generalised) for this outcome (P = 0.02). However, misclassification of seizure type for up to 48 individuals (32% of those with generalised epilepsy) may have confounded the results of this review. Despite concerns over side effects leading to the withdrawal of phenytoin as a first-line treatment in the USA and Europe, we found no evidence that phenytoin is more likely to be associated with serious side effects than carbamazepine; 26 individuals withdrew from 290 randomised (9%) to carbamazepine due to adverse effects, compared to 12 out of 299 (4%) randomised to phenytoin from four studies conducted in the USA and Europe (risk ratio (RR) 1.42, 95% CI 1.13 to 1.80, P = 0.014). We rated the quality of the evidence as low to moderate according to GRADE criteria, due to imprecision and potential misclassification of seizure type.
Authors' conclusions: We have not found evidence for a statistically significant difference between carbamazepine and phenytoin for the efficacy outcomes examined in this review, but CIs are wide and we cannot exclude the possibility of important differences. There is no evidence in this review that phenytoin is more strongly associated with serious adverse events than carbamazepine. There is some evidence that people with generalised seizures may be less likely to withdraw early from phenytoin than from carbamazepine, but misclassification of seizure type may have impacted upon our results. We recommend caution when interpreting the results of this review, and do not recommend that our results alone should be used in choosing between carbamazepine and phenytoin. We recommend that future trials should be designed to the highest quality possible, with considerations of allocation concealment and masking, choice of population, choice of outcomes and analysis, and presentation of results.
Conflict of interest statement
Sarah J Nevitt: none known
Anthony G Marson: A consortium of pharmaceutical companies (GSK, EISAI, UCB Pharma) funded the National Audit of Seizure Management in Hospitals (NASH) through grants paid to University of Liverpool. Professor Tony Marson is Theme Leader for Managing Complex Needs at NIHR CLAHRC NWC.
Jennifer Weston: none known
Catrin Tudur Smith: none known
Figures







Update of
-
Carbamazepine versus phenytoin monotherapy for epilepsy: an individual participant data review.Cochrane Database Syst Rev. 2015 Aug 14;(8):CD001911. doi: 10.1002/14651858.CD001911.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2017 Feb 27;2:CD001911. doi: 10.1002/14651858.CD001911.pub3. PMID: 26275105 Updated.
References
References to studies included in this review
-
- Callaghan N, Kenny RA, O'Neill B, Crowley M, Goggin T. A comparative study between carbamazepine, phenytoin and sodium valproate as monotherapy in previously untreated and recently diagnosed patients with epilepsy. British Journal of Clinical Practice 1983;27:7‐9. - PMC - PubMed
- Callaghan N, Kenny RA, O'Neill B, Crowley M, Goggin T. A prospective study between carbamazepine, phenytoin and sodium valproate as monotherapy in previously untreated and recently diagnosed patients with epilepsy. Journal of Neurology, Neurosurgery, and Psychiatry 1985;48(7):639‐44. - PMC - PubMed
- Goggin T, Casey C, Callaghan N. Serum levels of sodium valproate, phenytoin and carbamazepine and seizure control in epilepsy. Irish Medical Journal 1986;79(6):150‐6. - PubMed
-
- Czapinski P, Terczynski A, Czapinska E. Randomised 36‐month comparative study of valproic acid, phenytoin, phenobarbital and carbamazepine efficacy in patients with newly diagnosed epilepsy with partial complex seizures. Epilepsia 1997;38 Suppl(3):42.
-
- Silva M, MacArdle B, McGowan M, Hughes E, Stewart J, Neville BG, et al. Randomised comparative monotherapy trial of phenobarbitone, phenytoin, carbamazepine or sodium valproate for newly diagnosed childhood epilepsy. Lancet 1996;347(9003):709‐13. - PubMed
-
- Berg I, Butler A, Ellis M, Foster J. Psychiatric aspects of epilepsy in childhood treated with carbamazepine, phenytoin or sodium valproate: a random trial. Developmental Medicine and Child Neurology 1993;35(2):149‐57. - PubMed
- Forsythe I, Butler R, Berg I, McGuire R. Cognitive impairment in new cases of epilepsy randomly assigned to carbamazepine, phenytoin and sodium valproate. Developmental Medicine and Child Neurology 1991;33(6):524‐34. - PubMed
References to studies excluded from this review
-
- Bird CA, Griffin BP, Miklaszewska JM, Galbraith AW. Tegretol (carbamazepine): a controlled trial of new anti‐convulsant. British Journal of Psychiatry 1966;112:737‐42.
-
- Bittencourt PR, Antoniuk SA, Bigarella MM, Costa JC, Doro MP, Ferreira AS, et al. Carbamazepine and phenytoin in epilepsies refractory to barbiturates: efficacy, toxicity and mental function. Epilepsy Research 1993;16(2):147‐55. - PubMed
-
- Bawden HN, Camfield CS, Camfield PR, Cunningham C, Darwish H, Dooley JM, et al. The cognitive and behavioural effects of clobazam and standard monotherapy are comparable. Canadian Study Group for Childhood Epilepsy. Epilepsy Research 1999;33(2‐3):133‐43. - PubMed
- Canadian Study Group for Epilepsy. Clobazam has equivalent efficacy to carbamazepine and phenytoin as monotherapy for childhood epilepsy. Epilepsia 1998;39(9):952‐9. - PubMed
-
- Hakami T, Todaro M, Petrovski S, MacGregor L, Velakoulis D, Tan M, et al. Substitution monotherapy with levetiracetam vs older antiepileptic drugs: A randomized comparative trial. Archives of Neurology 2012;69(12):1563‐71. - PubMed
-
- Kaminow L, Schimschock JR, Hammer AE, Vuong A. Lamotrigine monotherapy compared with carbamazepine, phenytoin, or valproate monotherapy in patients with epilepsy. Epilepsy and Behaviour 2003;4(6):659‐66. - PubMed
- Martinez W, Kaminow L, Nanry KP, Hammer AE, Barrett PS. Evaluation of lamotrigine versus carbamazepine, phenytoin, or divalproex sodium as monotherapy for epilepsy patients who failed or could not tolerate previous antiepileptic drug therapy. Epilepsia 2000;41(Suppl 7):100.
References to studies awaiting assessment
-
- Rysz A. Effect of monotherapy with phenytoin or carbamazepine on somatosensory evoked potentials in patients with newly diagnosed epilepsy. Polski Tygodnik Lekarski 1994;49:79‐81. - PubMed
Additional references
-
- Annegers JF, Dubinsky S, Coan SP, Newmark ME, Roht L. The incidence of epilepsy and unprovoked seizures in multiethnic, urban health maintenance organizations. Epilepsia 1999;40(4):502‐6. - PubMed
-
- Carl GF, Smith ML. Phenytoin‐folate interactions: differing effects of the sodium salt and the free acid of phenytoin. Epilepsia 1992;33(2):372‐5. - PubMed
-
- Cockerell OC, Johnson AL, Sander JW, Hart YM, Shorvon SD. Remission of epilepsy: results from the National General Practice Study of Epilepsy. Lancet 1995;346(8968):140‐4. - PubMed
-
- Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 1981;22(4):489‐501. - PubMed
-
- Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia 1989;30(4):389‐99. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources