

Oxandrolone Coadministration Does Not Alter Plasma Propranolol Concentrations in Severely Burned Pediatric Patients
- PMID: 28240622
- PMCID: PMC5507814
- DOI: 10.1097/BCR.0000000000000494
Oxandrolone Coadministration Does Not Alter Plasma Propranolol Concentrations in Severely Burned Pediatric Patients
Abstract
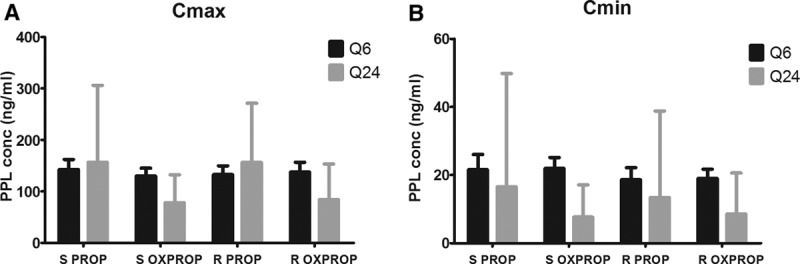
The systemic impact of severe burn injury results in a variety of disorders that require therapeutic intervention. Propranolol, a nonselective β1, β2-adrenergic receptor antagonist, reduces resting heart rate and cardiac work caused by elevated circulating catecholamines. Oxandrolone, a testosterone mimetic, promotes protein synthesis and anabolism to counter muscle wasting. Coadministration of these drugs is expected to synergistically improve patient outcomes. Testosterone administration is known to alter β-adrenergic receptor-mediated signaling. Here, we determined whether the coadministration of oxandrolone alters plasma propranolol concentrations. Ninety-two pediatric patients with burns covering ≥30% of the TBSA were enrolled in this institutional review board-approved study and randomized to receive propranolol (n = 49) or oxandrolone + propranolol (n = 43). Plasma propranolol concentrations were determined following two dosing strategies: Q6 (liquid formulation; n = 86) and Q24 (extended-release capsule; n = 22). Samples were drawn before drug administration and at regular intervals throughout the next two dosing periods. Heart rate and blood pressure were recorded throughout the study. Propranolol half-life was 3.3 hours for the Q6 drug dosing frequency (P < .0001) and 11.2 hours for the Q24 strategy (P < .0001). Percentage of predicted heart rate declined by 2.8% for each doubling of the propranolol concentration in the Q6 dosing schedule (P < .0001). Percentage of predicted heart rate declined by 2.5% for each doubling of propranolol concentration on the Q24 dosing schedule (P < .0001). Maximum and minimum propranolol plasma concentrations were similar with either dosing regimen. The addition of oxandrolone did not affect any of the measured parameters. Oxandrolone coadministration does not alter propranolol's plasma concentration, half-life, or effect on heart rate. This study is registered at clincialtrials.gov: NCT00675714.
Figures




Similar articles
-
Reduced Postburn Hypertrophic Scarring and Improved Physical Recovery With Yearlong Administration of Oxandrolone and Propranolol.Ann Surg. 2018 Sep;268(3):431-441. doi: 10.1097/SLA.0000000000002926. Ann Surg. 2018. PMID: 30048322 Free PMC article. Clinical Trial.
-
Reversal of Growth Arrest With the Combined Administration of Oxandrolone and Propranolol in Severely Burned Children.Ann Surg. 2016 Sep;264(3):421-8. doi: 10.1097/SLA.0000000000001844. Ann Surg. 2016. PMID: 27433905 Free PMC article. Clinical Trial.
-
Propranolol kinetics in plasma from severely burned adults.Burns. 2017 Sep;43(6):1168-1174. doi: 10.1016/j.burns.2016.10.019. Epub 2017 Jun 20. Burns. 2017. PMID: 28645713 Free PMC article. Clinical Trial.
-
Effects of pharmacological interventions on muscle protein synthesis and breakdown in recovery from burns.Burns. 2015 Jun;41(4):649-57. doi: 10.1016/j.burns.2014.10.010. Epub 2014 Nov 16. Burns. 2015. PMID: 25468473 Free PMC article. Review.
-
The pharmacologic modulation of the hypermetabolic response to burns.Adv Surg. 2005;39:245-61. doi: 10.1016/j.yasu.2005.05.005. Adv Surg. 2005. PMID: 16250555 Review.
Cited by
-
The efficacy and safety of androgen analog oxandrolone in improving clinical outcomes in burn patients: a systematic review and meta-analysis of randomized controlled trials.Front Med (Lausanne). 2025 Aug 8;12:1485474. doi: 10.3389/fmed.2025.1485474. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40861228 Free PMC article.
-
Anabolic and anticatabolic agents used in burn care: What is known and what is yet to be learned.Burns. 2020 Feb;46(1):19-32. doi: 10.1016/j.burns.2018.03.009. Epub 2019 Dec 15. Burns. 2020. PMID: 31852612 Free PMC article. Review.
-
Reduced Postburn Hypertrophic Scarring and Improved Physical Recovery With Yearlong Administration of Oxandrolone and Propranolol.Ann Surg. 2018 Sep;268(3):431-441. doi: 10.1097/SLA.0000000000002926. Ann Surg. 2018. PMID: 30048322 Free PMC article. Clinical Trial.
-
Application of beta-blockers in burn management.Proc (Bayl Univ Med Cent). 2021 Nov 22;35(1):46-50. doi: 10.1080/08998280.2021.2002110. eCollection 2022. Proc (Bayl Univ Med Cent). 2021. PMID: 34970031 Free PMC article.
References
-
- Abdullahi A, Jeschke MG. Nutrition and anabolic pharmacotherapies in the care of burn patients. Nutr Clin Pract 2014;29:621–30.. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
