

Multicenter, Phase III, Randomized, Double-Blind, Placebo-Controlled Trial of Pravastatin Added to First-Line Standard Chemotherapy in Small-Cell Lung Cancer (LUNGSTAR)
- PMID: 28240967
- PMCID: PMC5455702
- DOI: 10.1200/JCO.2016.69.7391
Multicenter, Phase III, Randomized, Double-Blind, Placebo-Controlled Trial of Pravastatin Added to First-Line Standard Chemotherapy in Small-Cell Lung Cancer (LUNGSTAR)
Abstract
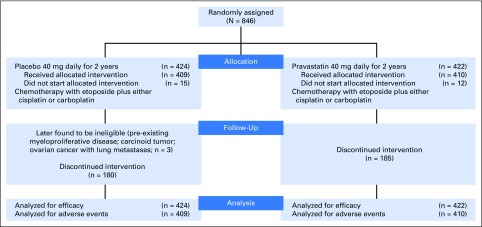
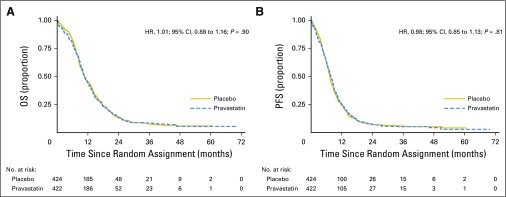
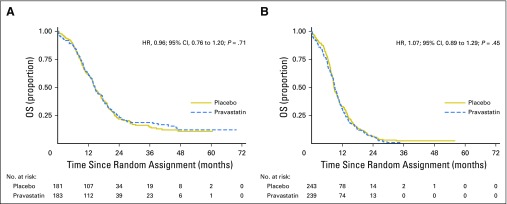
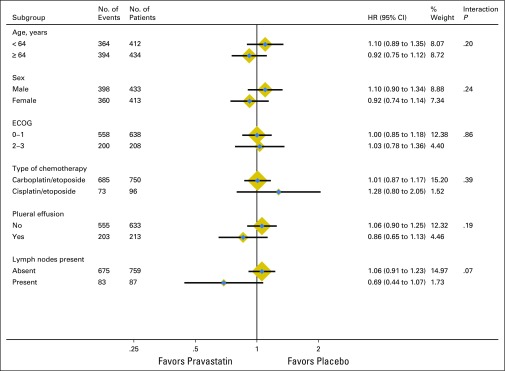
Purpose Treating small-cell lung cancer (SCLC) remains a therapeutic challenge. Experimental studies show that statins exert additive effects with agents, such as cisplatin, to impair tumor growth, and observational studies suggest that statins combined with anticancer therapies delay relapse and prolong life in several cancer types. To our knowledge, we report the first large, randomized, placebo-controlled, double-blind trial of a statin with standard-of-care for patients with cancer, specifically SCLC. Patients and Methods Patients with confirmed SCLC (limited or extensive disease) and performance status 0 to 3 were randomly assigned to receive daily pravastatin 40 mg or placebo, combined with up to six cycles of etoposide plus cisplatin or carboplatin every 3 weeks, until disease progression or intolerable toxicity. Primary end point was overall survival (OS), and secondary end points were progression-free survival (PFS), response rate, and toxicity. Results Eight hundred forty-six patients from 91 United Kingdom hospitals were recruited. The median age of recruited patients was 64 years of age, 43% had limited disease, and 57% had extensive disease. There were 758 deaths and 787 PFS events. No benefit was found for pravastatin, either in all patients or in several subgroups. For pravastatin versus placebo, the 2-year OS rate was 13.2% (95% CI, 10.0 to 16.7) versus 14.1% (95% CI, 10.9 to 17.7), respectively, with a hazard ratio of 1.01 (95% CI, 0.88 to 1.16; P = .90. The median OS was 10.7 months v 10.6 months, respectively. The median PFS was 7.7 months v 7.3 months, respectively. The median OS (pravastatin v placebo) was 14.6 months in both groups for limited disease and 9.1 months versus 8.8 months, respectively, for extensive disease. Adverse events were similar between groups. Conclusion Pravastatin 40 mg combined with standard SCLC therapy, although safe, does not benefit patients. Our conclusions are the same as those found in all four much smaller, randomized, placebo-controlled trials specifically designed to evaluate statin therapy in patients with cancer.
Figures
Comment in
-
Do Statins Improve Survival in Small-Cell Lung Cancer?J Clin Oncol. 2017 May 10;35(14):1497-1498. doi: 10.1200/JCO.2016.72.0870. Epub 2017 Mar 6. J Clin Oncol. 2017. PMID: 28475851 No abstract available.
-
No room for statins in the quest for survival benefits in small cell lung cancer.Transl Lung Cancer Res. 2018 Apr;7(Suppl 2):S131-S133. doi: 10.21037/tlcr.2018.03.07. Transl Lung Cancer Res. 2018. PMID: 29780705 Free PMC article. No abstract available.
References
-
- Fulcher J, O’Connell R, Voysey M, et al. Efficacy and safety of LDL-lowering therapy among men and women: Meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet. 2015;385:1397–1405. - PubMed
-
- Müller C, Bockhorn A. G., Klusmeier S, et al. Lovastatin inhibits proliferation of pancreatic cancer cell lines with mutant as well as with wild-type K-ras oncogene but has different effects on protein phosphorylation and induction of apoptosis. Int J Oncol. 1998;12:717–723. - PubMed
-
- Rubins JB, Greatens T, Kratzke RA, et al. Lovastatin induces apoptosis in malignant mesothelioma cells. Am J Respir Crit Care Med. 1998;157:1616–1622. - PubMed
-
- Kozar K, Kaminski R, Legat M, et al. Cerivastatin demonstrates enhanced antitumor activity against human breast cancer cell lines when used in combination with doxorubicin or cisplatin. Int J Oncol. 2004;24:1149–1157. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
