

The burden of typhoid fever in low- and middle-income countries: A meta-regression approach
- PMID: 28241011
- PMCID: PMC5344533
- DOI: 10.1371/journal.pntd.0005376
The burden of typhoid fever in low- and middle-income countries: A meta-regression approach
Abstract
Background: Upcoming vaccination efforts against typhoid fever require an assessment of the baseline burden of disease in countries at risk. There are no typhoid incidence data from most low- and middle-income countries (LMICs), so model-based estimates offer insights for decision-makers in the absence of readily available data.
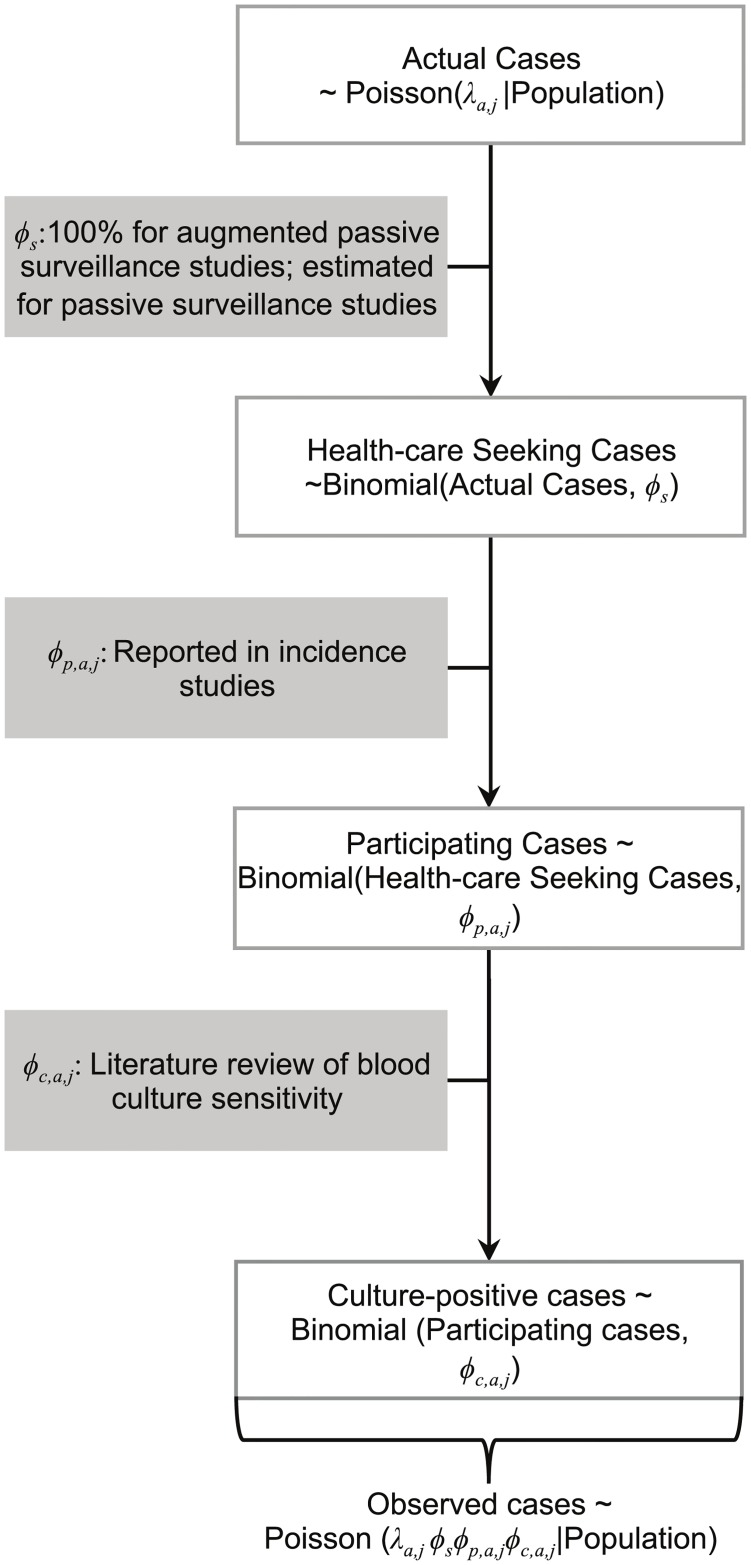
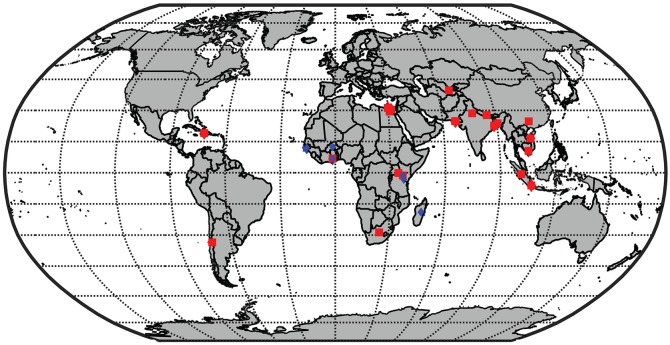
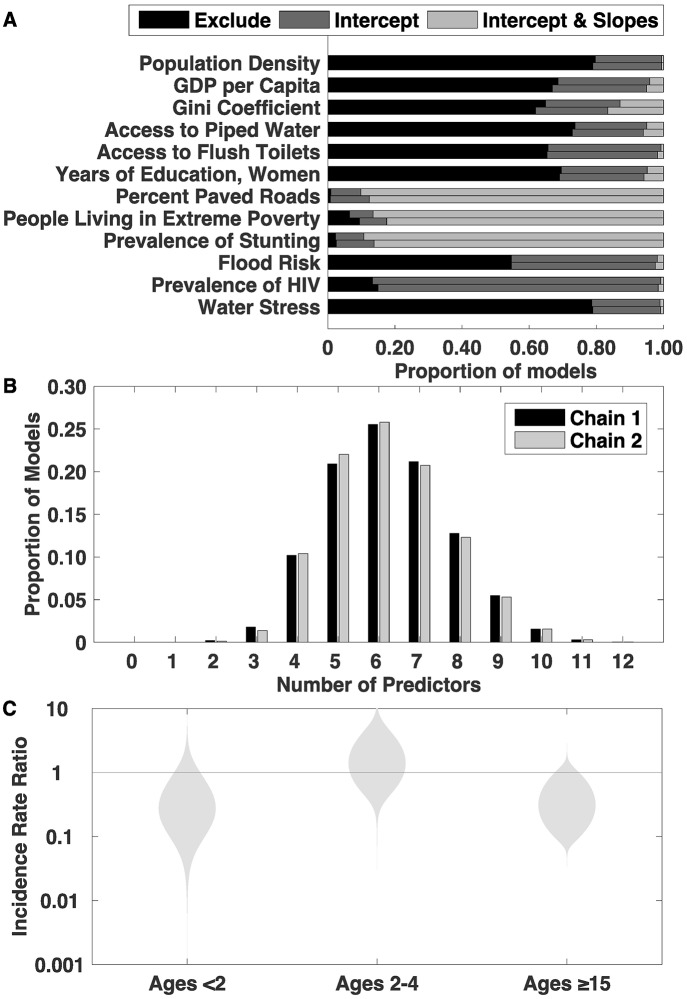
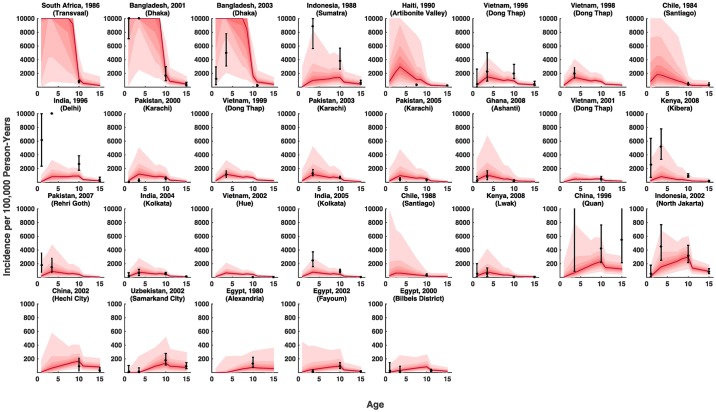
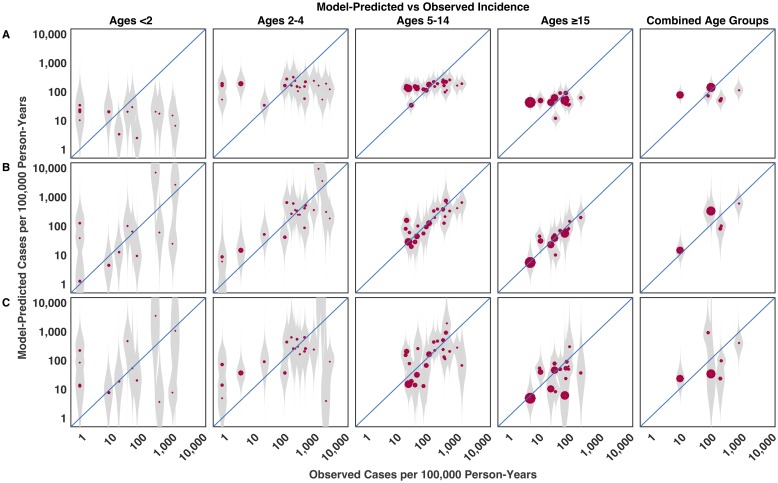
Methods: We developed a mixed-effects model fit to data from 32 population-based studies of typhoid incidence in 22 locations in 14 countries. We tested the contribution of economic and environmental indices for predicting typhoid incidence using a stochastic search variable selection algorithm. We performed out-of-sample validation to assess the predictive performance of the model.
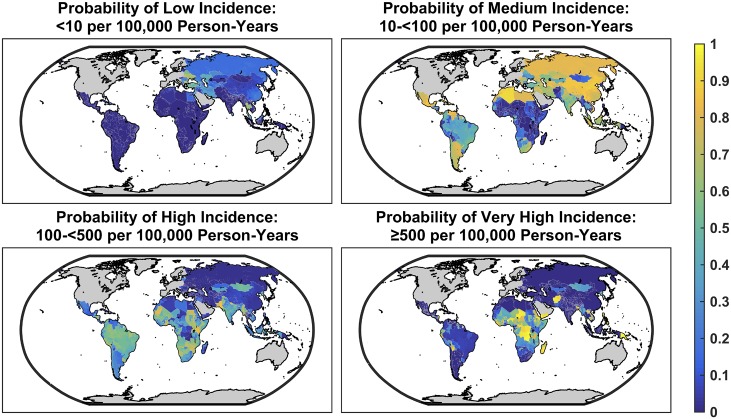
Results: We estimated that 17.8 million cases of typhoid fever occur each year in LMICs (95% credible interval: 6.9-48.4 million). Central Africa was predicted to experience the highest incidence of typhoid, followed by select countries in Central, South, and Southeast Asia. Incidence typically peaked in the 2-4 year old age group. Models incorporating widely available economic and environmental indicators were found to describe incidence better than null models.
Conclusions: Recent estimates of typhoid burden may under-estimate the number of cases and magnitude of uncertainty in typhoid incidence. Our analysis permits prediction of overall as well as age-specific incidence of typhoid fever in LMICs, and incorporates uncertainty around the model structure and estimates of the predictors. Future studies are needed to further validate and refine model predictions and better understand year-to-year variation in cases.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Mogasale V, Maskery B, Ochiai RL, Lee JS, Mogasale V V, Ramani E, et al. Burden of typhoid fever in low-income and middle-income countries: a systematic, literature-based update with risk-factor adjustment. Lancet Glob Heal; 2014;2: e570–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
