

Analysis of Mycobacterium ulcerans-specific T-cell cytokines for diagnosis of Buruli ulcer disease and as potential indicator for disease progression
- PMID: 28241036
- PMCID: PMC5344519
- DOI: 10.1371/journal.pntd.0005415
Analysis of Mycobacterium ulcerans-specific T-cell cytokines for diagnosis of Buruli ulcer disease and as potential indicator for disease progression
Abstract
Background: Buruli ulcer disease (BUD), caused by Mycobacterium (M.) ulcerans, is the third most common mycobacterial disease after tuberculosis and leprosy. BUD causes necrotic skin lesions and is a significant problem for health care in the affected countries. As for other mycobacterial infections, T cell mediated immune responses are important for protection and recovery during treatment, but detailed studies investigating these immune responses in BUD patients are scarce. In this study, we aimed to characterise M. ulcerans-specific CD4+ T cell responses in BUD patients and to analyse specific cytokine-producing T cells in the context of disease severity and progression.
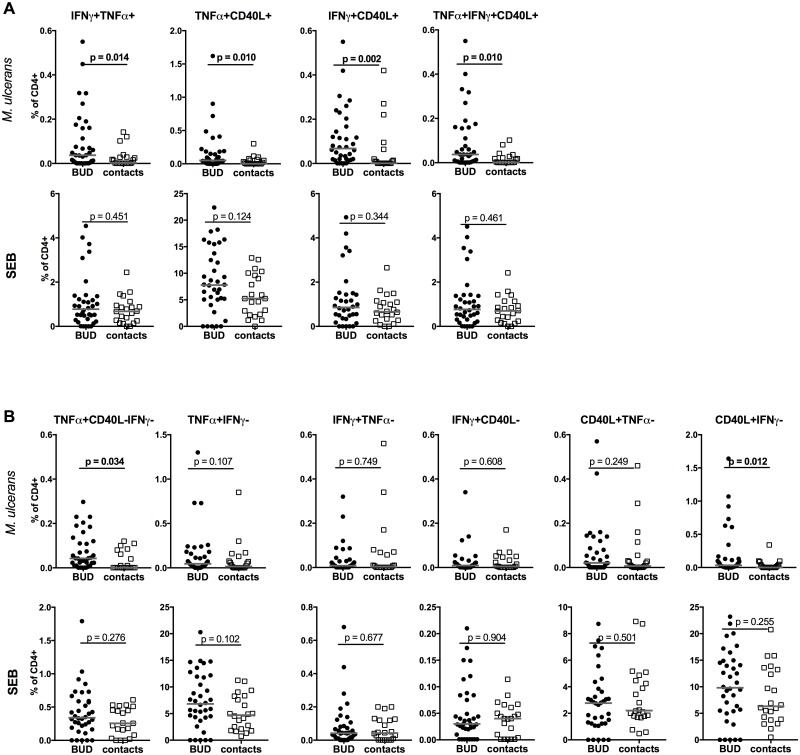
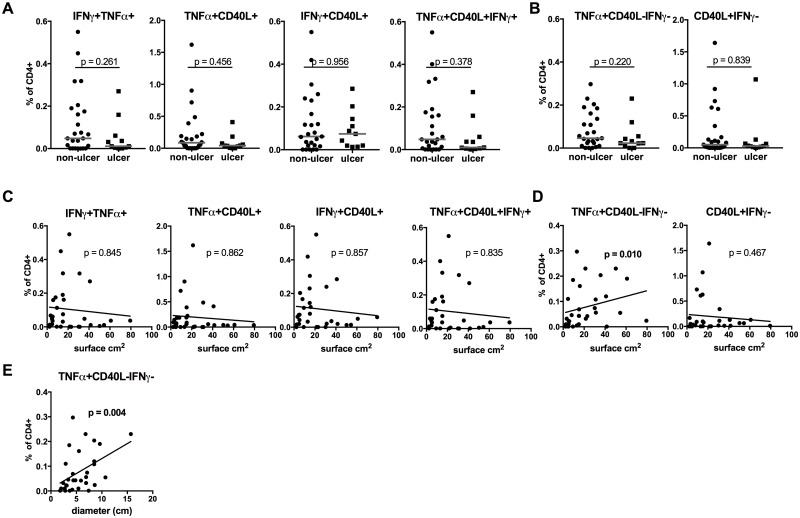
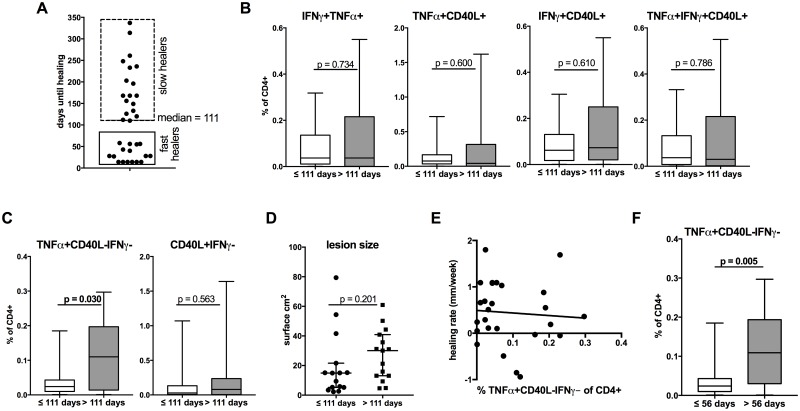
Methodology/principal findings: For this case-control study, whole blood samples of BUD patients (N = 36, 1.5-17 years of age) and healthy contacts (N = 22, 3-15 years of age) were stimulated with antigen prepared from M. ulcerans and CD4+ T cells were analysed for the expression of TNFα, IFNγ and CD40L by flow cytometry. The proportions and profile of cytokine producing CD4+ T cells was compared between the two study groups and correlated with disease progression and severity. Proportions of cytokine double-positive IFNγ+TNFα+, TNFα+CD40L+, IFNγ+CD40L+ (p = 0.014, p = 0.010, p = 0.002, respectively) and triple positive IFNγ+TNFα+CD40L+ (p = 0.010) producing CD4+ T cell subsets were increased in BUD patients. In addition, TNFα+CD40L-IFNγ- CD4+ T cells differed between patients and controls (p = 0.034). TNFα+CD40L-IFNγ- CD4+ T cells were correlated with lesion size (p = 0.010) and proportion were higher in 'slow' healers compared to 'fast healers' (p = 0.030).
Conclusions: We were able to identify M. ulcerans-specific CD4+ T cell subsets with specific cytokine profiles. In particular a CD4+ T cell subset, producing TNFα but not IFNγ and CD40L, showed association with lesion size and healing progress. Further studies are required to investigate, if the identified CD4+ T cell subset has the potential to be used as biomarker for diagnosis, severity and/or progression of disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Memory B-cells are enriched in the blood of patients with acute Buruli ulcer disease: a prospective observational study.BMC Infect Dis. 2023 Jun 12;23(1):393. doi: 10.1186/s12879-023-08370-1. BMC Infect Dis. 2023. PMID: 37308884 Free PMC article.
-
Immunosuppressive signature of cutaneous Mycobacterium ulcerans infection in the peripheral blood of patients with buruli ulcer disease.J Infect Dis. 2009 Dec 1;200(11):1675-84. doi: 10.1086/646615. J Infect Dis. 2009. PMID: 19863437
-
T-Cell Responses Against Mycobacterium ulcerans and Mycobacterium tuberculosis Protein Extracts Identify Children With Buruli Ulcer Disease.J Pediatric Infect Dis Soc. 2022 Dec 28;11(12):575-577. doi: 10.1093/jpids/piac092. J Pediatric Infect Dis Soc. 2022. PMID: 36070406
-
Cell-mediated and serology-based tests for Mycobacterium ulcerans disease: A systematic review and meta-analysis.PLoS Negl Trop Dis. 2020 Apr 6;14(4):e0008172. doi: 10.1371/journal.pntd.0008172. eCollection 2020 Apr. PLoS Negl Trop Dis. 2020. PMID: 32251470 Free PMC article.
-
Buruli ulcer: Advances in understanding Mycobacterium ulcerans infection.Dermatol Clin. 2011 Jan;29(1):1-8. doi: 10.1016/j.det.2010.09.006. Dermatol Clin. 2011. PMID: 21095521 Review.
Cited by
-
Memory B-cells are enriched in the blood of patients with acute Buruli ulcer disease: a prospective observational study.BMC Infect Dis. 2023 Jun 12;23(1):393. doi: 10.1186/s12879-023-08370-1. BMC Infect Dis. 2023. PMID: 37308884 Free PMC article.
-
A human model of Buruli ulcer: Provisional protocol for a Mycobacterium ulcerans controlled human infection study.Wellcome Open Res. 2024 Oct 21;9:488. doi: 10.12688/wellcomeopenres.22719.2. eCollection 2024. Wellcome Open Res. 2024. PMID: 39386965 Free PMC article.
-
The One That Got Away: How Macrophage-Derived IL-1β Escapes the Mycolactone-Dependent Sec61 Blockade in Buruli Ulcer.Front Immunol. 2022 Jan 26;12:788146. doi: 10.3389/fimmu.2021.788146. eCollection 2021. Front Immunol. 2022. PMID: 35154073 Free PMC article.
-
Evaluation of an electricity-independent method for IS2404 Loop-mediated isothermal amplification (LAMP) diagnosis of Buruli ulcer in resource-limited settings.PLoS Negl Trop Dis. 2024 Aug 14;18(8):e0012338. doi: 10.1371/journal.pntd.0012338. eCollection 2024 Aug. PLoS Negl Trop Dis. 2024. PMID: 39141676 Free PMC article.
-
Identification and validation of host biomarkers for leprosy: A step forward to establish point-of-care tests.EBioMedicine. 2019 Oct;48:9-10. doi: 10.1016/j.ebiom.2019.09.028. Epub 2019 Oct 17. EBioMedicine. 2019. PMID: 31631045 Free PMC article. No abstract available.
References
-
- World Health Organization. Buruli ulcer—Fact sheet No199 Geneva: 2016; 2016 [cited 2016 08/2016]. http://www.who.int/mediacentre/factsheets/fs199/en/.
-
- Schunk M, Thompson W, Klutse E, Nitschke J, Opare-Asamoah K, Thompson R, et al. Outcome of patients with buruli ulcer after surgical treatment with or without antimycobacterial treatment in Ghana. Am J Trop Med Hyg. 2009;81(1):75–81. - PubMed
-
- World Health Organization. Buruli Ulcer: Prevention of Disability (POD). Manual for Health Care Providers Geneva2009 [cited 2016 08/2016]. http://www.who.int/buruli/information/publications/BU-0POD-presentation.pdf.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
