

Early recognition of multiple sclerosis using natural language processing of the electronic health record
- PMID: 28241760
- PMCID: PMC5329909
- DOI: 10.1186/s12911-017-0418-4
Early recognition of multiple sclerosis using natural language processing of the electronic health record
Abstract
Background: Diagnostic accuracy might be improved by algorithms that searched patients' clinical notes in the electronic health record (EHR) for signs and symptoms of diseases such as multiple sclerosis (MS). The focus this study was to determine if patients with MS could be identified from their clinical notes prior to the initial recognition by their healthcare providers.
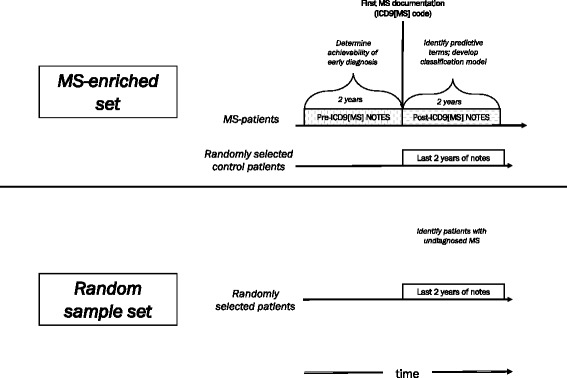
Methods: An MS-enriched cohort of patients with well-established MS (n = 165) and controls (n = 545), was generated from the adult outpatient clinic. A random sample cohort was generated from randomly selected patients (n = 2289) from the same adult outpatient clinic, some of whom had MS (n = 16). Patients' notes were extracted from the data warehouse and signs and symptoms mapped to UMLS terms using MedLEE. Approximately 1000 MS-related terms occurred significantly more frequently in MS patients' notes than controls'. Synonymous terms were manually clustered into 50 buckets and used as classification features. Patients were classified as MS or not using Naïve Bayes classification.
Results: Classification of patients known to have MS using notes of the MS-enriched cohort entered after the initial ICD9[MS] code yielded an ROC AUC, sensitivity, and specificity of 0.90 [0.87-0.93], 0.75[0.66-0.82], and 0.91 [0.87-0.93], respectively. Similar classification accuracy was achieved using the notes from the random sample cohort. Classification of patients not yet known to have MS using notes of the MS-enriched cohort entered before the initial ICD9[MS] documentation identified 40% [23-59%] as having MS. Manual review of the EHR of 45 patients of the random sample cohort classified as having MS but lacking an ICD9[MS] code identified four who might have unrecognized MS.
Conclusions: Diagnostic accuracy might be improved by mining patients' clinical notes for signs and symptoms of specific diseases using NLP. Using this approach, we identified patients with MS early in the course of their disease which could potentially shorten the time to diagnosis. This approach could also be applied to other diseases often missed by primary care providers such as cancer. Whether implementing computerized diagnostic support ultimately shortens the time from earliest symptoms to formal recognition of the disease remains to be seen.
Keywords: Computer-assisted [E01.158]; Diagnosis; Diagnostic errors [E01.354]; Early Diagnosis [E01.390]; Electronic health records [E05.318.308.940.968.249.500]; Natural language processing [L01.224.050.375.580]; multiple sclerosis [C10.114.375.500].
Figures
References
-
- Committee on Diagnostic Error in Health Care BoHCS, Institute of Medicine, The National Academies of Sciences, Engineering, and Medicine . Improving diagnosis in health care. Washington (DC): National Academies Press (US); 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
