

Effects of canagliflozin, a sodium glucose co-transporter 2 inhibitor, on blood pressure and markers of arterial stiffness in patients with type 2 diabetes mellitus: a post hoc analysis
- PMID: 28241822
- PMCID: PMC5327537
- DOI: 10.1186/s12933-017-0511-0
Effects of canagliflozin, a sodium glucose co-transporter 2 inhibitor, on blood pressure and markers of arterial stiffness in patients with type 2 diabetes mellitus: a post hoc analysis
Abstract
Background: Physiologic determinants, such as pulse pressure [difference between systolic blood pressure (SBP) and diastolic BP (DBP)], mean arterial pressure (2/3 DBP + 1/3 SBP), and double product [beats per minute (bpm) × SBP], are linked to cardiovascular outcomes. The effects of canagliflozin, a sodium glucose co-transporter 2 (SGLT2) inhibitor, on pulse pressure, mean arterial pressure, and double product were assessed in patients with type 2 diabetes mellitus (T2DM).
Methods: This post hoc analysis was based on pooled data from four 26-week, randomized, double-blind, placebo-controlled studies evaluating canagliflozin in patients with T2DM (N = 2313) and a 6-week, randomized, double-blind, placebo-controlled, ambulatory BP monitoring (ABPM) study evaluating canagliflozin in patients with T2DM and hypertension (N = 169). Changes from baseline in SBP, DBP, pulse pressure, mean arterial pressure, and double product were assessed using seated BP measurements (pooled studies) or averaged 24-h BP assessments (ABPM study). Safety was assessed based on adverse event reports.
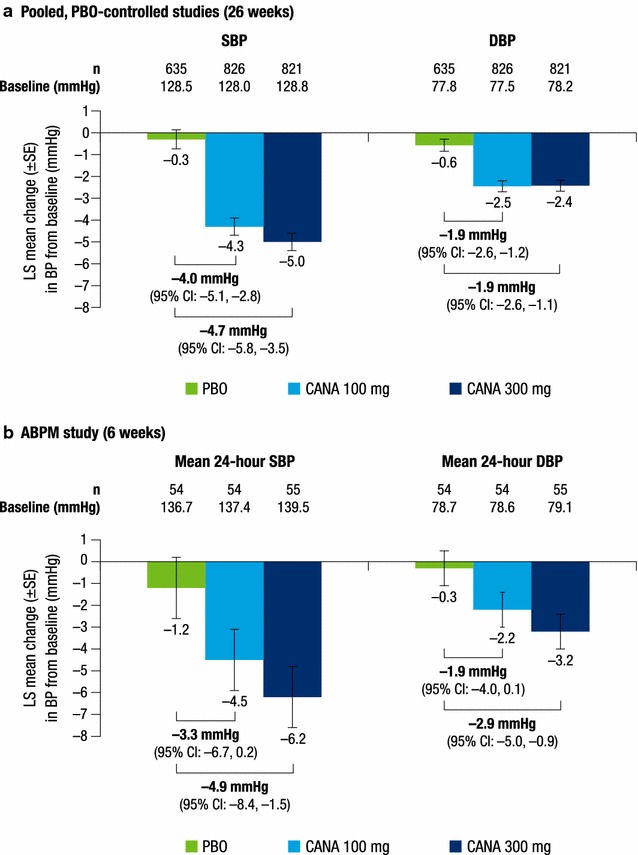
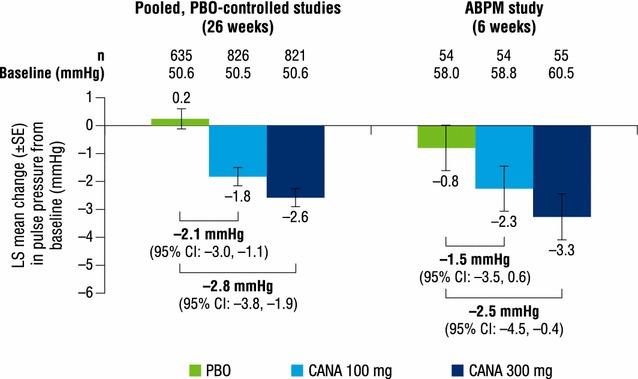
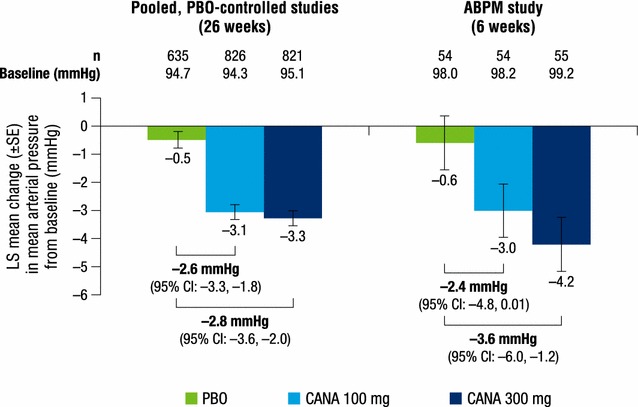
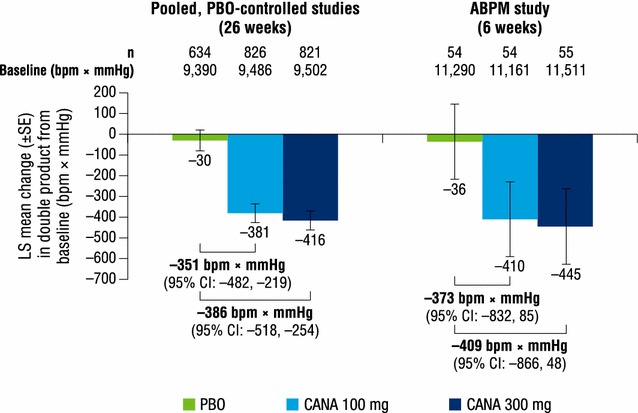
Results: In the pooled studies, canagliflozin 100 and 300 mg reduced SBP (-4.3 and -5.0 vs -0.3 mmHg) and DBP (-2.5 and -2.4 vs -0.6 mmHg) versus placebo at week 26. Reductions in pulse pressure (-1.8 and -2.6 vs 0.2 mmHg), mean arterial pressure (-3.1 and -3.3 vs -0.5 mmHg), and double product (-381 and -416 vs -30 bpm × mmHg) were also seen with canagliflozin 100 and 300 mg versus placebo. In the ABPM study, canagliflozin 100 and 300 mg reduced mean 24-h SBP (-4.5 and -6.2 vs -1.2 mmHg) and DBP (-2.2 and -3.2 vs -0.3 mmHg) versus placebo at week 6. Canagliflozin 300 mg provided reductions in pulse pressure (-3.3 vs -0.8 mmHg) and mean arterial pressure (-4.2 vs -0.6 mmHg) compared with placebo, while canagliflozin 100 mg had more modest effects on these parameters. Canagliflozin was generally well tolerated in both study populations.
Conclusions: Canagliflozin improved all three cardiovascular physiologic markers, consistent with the hypothesis that canagliflozin may have beneficial effects on some cardiovascular outcomes in patients with T2DM. Trial registration ClinicalTrials.gov Identifier: NCT01081834 (registered March 2010); NCT01106677 (registered April 2010); NCT01106625 (registered April 2010); NCT01106690 (registered April 2010); NCT01939496 (registered September 2013).
Keywords: Ambulatory blood pressure monitoring; Blood pressure; Canagliflozin; Double product; Mean arterial pressure; Pulse pressure; Sodium glucose co-transporter 2 (SGLT2) inhibitor; Type 2 diabetes.
Figures
References
-
- American Diabetes Association Standards of medical care in diabetes–2016. Diabetes Care. 2016;39(suppl 1):S1–S108. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
