

The accuracy of transcranial Doppler in excluding intracranial hypertension following acute brain injury: a multicenter prospective pilot study
- PMID: 28241847
- PMCID: PMC5329967
- DOI: 10.1186/s13054-017-1632-2
The accuracy of transcranial Doppler in excluding intracranial hypertension following acute brain injury: a multicenter prospective pilot study
Abstract
Background: Untimely diagnosis of intracranial hypertension may lead to delays in therapy and worsening of outcome. Transcranial Doppler (TCD) detects variations in cerebral blood flow velocity which may correlate with intracranial pressure (ICP). We investigated if intracranial hypertension can be accurately excluded through use of TCD.
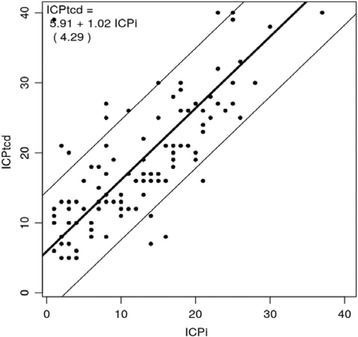
Method: This was a multicenter prospective pilot study in patients with acute brain injury requiring invasive ICP (ICPi) monitoring. ICP estimated with TCD (ICPtcd) was compared with ICPi in three separate time frames: immediately before ICPi placement, immediately after ICPi placement, and 3 hours following ICPi positioning. Sensitivity and specificity, and concordance correlation coefficient between ICPi and ICPtcd were calculated. Receiver operating curve (ROC) and the area under the curve (AUC) analyses were estimated after measurement averaging over time.
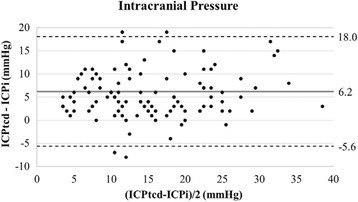
Results: A total of 38 patients were enrolled, and of these 12 (31.6%) had at least one episode of intracranial hypertension. One hundred fourteen paired measurements of ICPi and ICPtcd were gathered for analysis. With dichotomized ICPi (≤20 mmHg vs >20 mmHg), the sensitivity of ICPtcd was 100%; all measurements with high ICPi (>20 mmHg) also had a high ICPtcd values. Bland-Altman plot showed an overestimation of 6.2 mmHg (95% CI 5.08-7.30 mmHg) for ICPtcd compared to ICPi. AUC was 96.0% (95% CI 89.8-100%) and the estimated best threshold was at ICPi of 24.8 mmHg corresponding to a sensitivity 100% and a specificity of 91.2%.
Conclusions: This study provides preliminary evidence that ICPtcd may accurately exclude intracranial hypertension in patients with acute brain injury. Future studies with adequate power are needed to confirm this result.
Keywords: Brain injury; Intracranial hypertension; Intracranial pressure; Transcranial Doppler.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
