

Survival Gains from First-Line Systemic Therapy in Metastatic Non-Small Cell Lung Cancer in the U.S., 1990-2015: Progress and Opportunities
- PMID: 28242792
- PMCID: PMC5344635
- DOI: 10.1634/theoncologist.2016-0253
Survival Gains from First-Line Systemic Therapy in Metastatic Non-Small Cell Lung Cancer in the U.S., 1990-2015: Progress and Opportunities
Abstract
Background: Approximately 190,000 Americans are diagnosed with non-small cell lung cancer (NSCLC) annually, and about half have metastatic (Stage IV) disease. These patients have historically had poor survival prognosis, but several new therapies introduced since 2000 provide options for improved outcomes. The objectives of this study were to quantify survival gains from 1990, when best supportive care (BSC) only was standard, to 2015 and to estimate the impact of expanded use of systemic therapies in clinically appropriate patients.
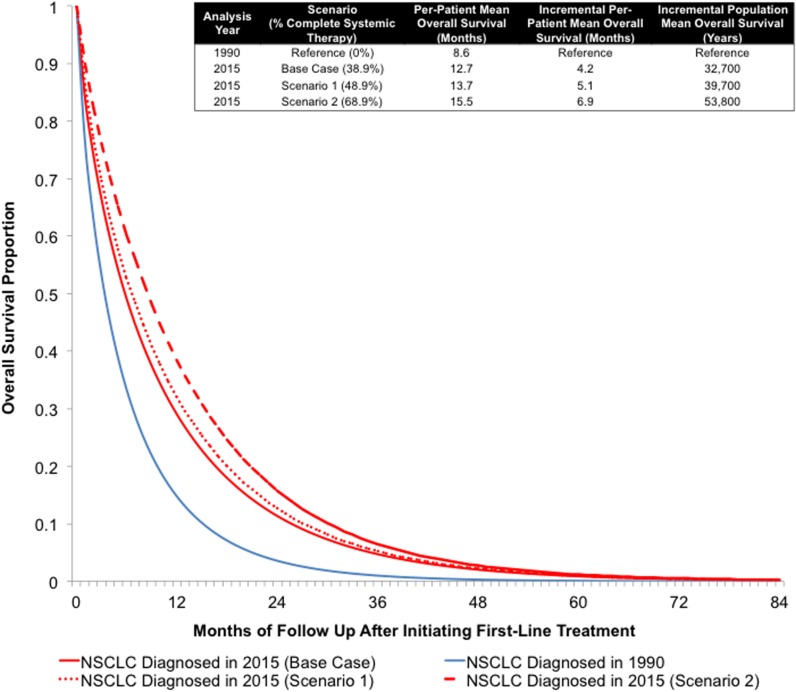
Materials and methods: We developed a simulation model to estimate survival gains for patients with metastatic NSCLC from 1990-2015. Survival estimates were derived from major clinical trials and extrapolated to a lifetime horizon. Proportions of patients receiving available therapies were derived from the Surveillance, Epidemiology, and End Results database and a commercial treatment registry. We also estimated gains in overall survival (OS) in scenarios in which systemic therapy use increased by 10% and 30% relative to current use.
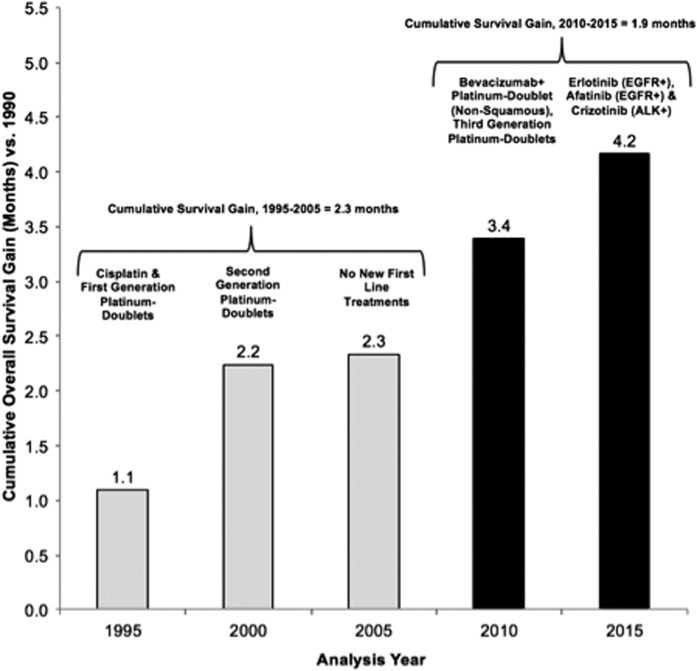
Results: From 1990-2015, one-year survival proportion increased by 14.1% and mean per-patient survival improved by 4.2 months (32,700 population life years). Increasing treated patients by 10% or 30% increased OS by 5.1 months (39,700 population life years) and 6.9 months (53,800 population life years), respectively.
Conclusion: Although survival remains poor in metastatic NSCLC relative to other common cancers, meaningful progress in per-patient and population-level outcomes has been realized over the past 25 years. These advances can be improved even further by increasing use of systemic therapies in the substantial proportion of patients who are suitable for treatment yet who currently receive BSC only. The Oncologist 2017;22:304-310 IMPLICATIONS FOR PRACTICE: Approximately 93,500 Americans are diagnosed with metastatic non-small cell lung cancer (NSCLC) annually. Historically, these patients have had poor survival prognosis, but newer therapies provide options for improved outcomes. This simulation modeling study quantified metastatic NSCLC survival gains from 1990-2015. Over this period, the one-year survival proportion and mean per-patient survival increased by 14.1% and 4.2 months, respectively. Though metastatic NSCLC survival remains poor, the past 25 years have brought meaningful gains. Additional gains could be realized by increasing systemic therapy use in the substantial proportion of patients who are suitable for treatment, yet currently receive only supportive care.
Keywords: Non‐small cell lung cancer; Overall survival; Systemic therapy.
© AlphaMed Press 2017.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65(1):5–29. - PubMed
-
- Howlader N NA, Krapcho M, Neyman N. et al (eds). SEER Cancer Statistics Review, 1975–2009. 2012; Available at http://seer.cancer.gov/csr/1975_2009_pops09/sections.html. Accessed August 23, 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
