Immediate Postoperative Intraocular Pressure Adjustment Reduces Risk of Cystoid Macular Edema after Uncomplicated Micro Incision Coaxial Phacoemulsification Cataract Surgery
- PMID: 28243022
- PMCID: PMC5327173
- DOI: 10.3341/kjo.2017.31.1.39
Immediate Postoperative Intraocular Pressure Adjustment Reduces Risk of Cystoid Macular Edema after Uncomplicated Micro Incision Coaxial Phacoemulsification Cataract Surgery
Abstract
Purpose: To determine the accuracy of visual estimation of immediate postoperative intraocular pressure (IOP) following microincision cataract surgery (MICS) and the effect of immediate postoperative IOP adjustment on prevention of cystoid macular edema (CME).
Setting: Ambulatory surgical center.
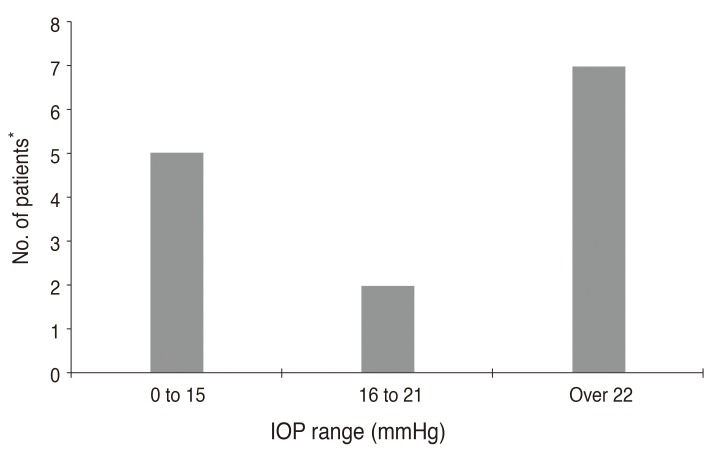
Methods: Prospective, randomized analysis of 170 eyes in 135 patients with MICS, performed in a Medicare approved outpatient ambulatory surgery center. Surgical parameters included a keratome incision of 1.5 mm to 2.8 mm, topical anesthetic, case completion IOP estimation by palpation and patient visualization of light, and IOP adjustment before exiting the operating theater. IOPs were classified into three groups: low (<16 mmHg), normal (16 to 21 mmHg), and elevated (>21 to 30 mmHg). IOP measurements were repeated 1 day after surgery. Optical coherence tomography (Stratus OCT, Zeiss) was measured at 2 weeks. An increase in foveal thickness greater than 15 µm was used to indicate CME. Statistical analysis was performed using one- and two-tailed Student's t-tests.
Results: Mean minimal foveal thickness averaged 207.15 µm in the low pressure group, 205.14 µm in the normal IOP group, and 210.48 µm in the elevated IOP group 2 weeks following surgery. CME occurred in 14 of 170 eyes (8.2%) at 2 weeks (low IOP, 35.7%; normal IOP, 14.2%; elevated IOP, 50.0%). Change in IOP from the operating theater to 1 day after surgery was within +/-5 mmHg in 54 eyes (31.7%), elevated by 6 to 15 mmHg in 22 eyes (12.9%), and elevated more than 15 mmHg in four eyes (2.3%). IOP was reduced by 6 mmHg to 15 mmHg in 39 eyes (22.9%) and reduced by more than 15 mmHg in nine eyes (5.3%).
Conclusions: Immediate postoperative adjustment of IOP may prevent CME in MICS. Physicians can improve their ability to estimate postoperative IOP with experience in tonometry to verify immediate postoperative IOP. There are patient safety and economic benefits to immediate IOP adjustment in the operating theater.
Synopsis: Immediate postoperative IOP adjustment following cataract surgery before the patient leaves the operating theater may reduce the incidence of CME and provide patient safety and economic benefits.
Keywords: CME; Cystoid; Edema; MICS; Pressure.
Conflict of interest statement
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Figures



Similar articles
-
Evaluation of cystoid macular edema using optical coherence tomography and fundus fluorescein angiography after uncomplicated phacoemulsification surgery.Curr Eye Res. 2012 Apr;37(4):327-33. doi: 10.3109/02713683.2011.635402. Curr Eye Res. 2012. PMID: 22440164 Clinical Trial.
-
Diclofenac prevents an early event of macular thickening after cataract surgery in patients with diabetes.J Ocul Pharmacol Ther. 2007 Jun;23(3):284-91. doi: 10.1089/jop.2006.134. J Ocul Pharmacol Ther. 2007. PMID: 17593013 Clinical Trial.
-
Prevalence of optical coherence tomography-diagnosed postoperative cystoid macular oedema in patients following uncomplicated phaco-emulsification cataract surgery.Clin Exp Ophthalmol. 2012 Apr;40(3):282-7. doi: 10.1111/j.1442-9071.2011.02638.x. Epub 2011 Sep 2. Clin Exp Ophthalmol. 2012. PMID: 21718410
-
Laser flare and cell photometry to measure inflammation after cataract surgery: a tool to predict the risk of cystoid macular edema.Int Ophthalmol. 2021 Jun;41(6):2293-2300. doi: 10.1007/s10792-021-01779-0. Epub 2021 Mar 21. Int Ophthalmol. 2021. PMID: 33745035 Review.
-
Postsurgical Cystoid Macular Edema.Dev Ophthalmol. 2017;58:178-190. doi: 10.1159/000455280. Epub 2017 Mar 28. Dev Ophthalmol. 2017. PMID: 28351047 Review.
Cited by
-
Do we need day-1 postoperative follow-up after cataract surgery?Graefes Arch Clin Exp Ophthalmol. 2019 May;257(5):855-861. doi: 10.1007/s00417-018-04210-0. Epub 2018 Dec 19. Graefes Arch Clin Exp Ophthalmol. 2019. PMID: 30569320 Review.
-
Toll-like receptor 3 gene regulates cataract-related mechanisms via the Jagged-1/Notch signaling pathway.Bioengineered. 2022 Jun;13(6):14357-14367. doi: 10.1080/21655979.2022.2085391. Bioengineered. 2022. PMID: 35758265 Free PMC article.
-
Is Palpation Sufficient for Estimation of IOP Immediately Following Cataract Surgery?Med Hypothesis Discov Innov Ophthalmol. 2020 Summer;9(2):143-148. Epub 2020 Mar 30. Med Hypothesis Discov Innov Ophthalmol. 2020. PMID: 32490021 Free PMC article.
-
Changes in Macular Thickness after Cataract Surgery in Patients with Open Angle Glaucoma.Diagnostics (Basel). 2023 Jan 9;13(2):244. doi: 10.3390/diagnostics13020244. Diagnostics (Basel). 2023. PMID: 36673054 Free PMC article.
-
Effect of microincisional cataract surgery on inflammatory indicators in tears and corneal endothelial cells in cataract patients.Am J Transl Res. 2021 Jul 15;13(7):7705-7714. eCollection 2021. Am J Transl Res. 2021. PMID: 34377247 Free PMC article.
References
-
- Jurecka T, Batkova Z, Ventruba J. Macular edema after an uncomplicated cataract surgery. Cesk Slov Oftalmol. 2007;63:262–273. - PubMed
-
- El-Ashry M, Hegde V, James P, Pagliarini S. Analysis of macular thickness in British population using optical coherence tomography (OCT): an emphasis on interocular symmetry. Curr Eye Res. 2008;33:693–699. - PubMed
-
- Kecik D, Makowiec-Tabernacka M, Golebiewska J, et al. Macular thickness and volume after uncomplicated phacoemulsification surgery evaluated by optical coherence tomography: a one-year follow-up. Neuro Endocrinol Lett. 2009;30:610–614. - PubMed
-
- Burling-Phillips L. After cataract surgery: watching for cystoid macular edema [Internet] San Francisco, CA: EyeNet; 2007. [cited 2017 Jan 13]. Available from: http://www.aao.org/publications/eyenet/200701/retina.cfm.
-
- Yuksel N, Dogu B, Karabas VL, Caglar Y. Foveal thickness after phacoemulsification in patients with pseudoexfoliation syndrome, pseudoexfoliation glaucoma, or primary open-angle glaucoma. J Cataract Refract Surg. 2008;34:1953–1957. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical