

Short Segment versus Long Segment Pedicle Screws Fixation in Management of Thoracolumbar Burst Fractures: Meta-Analysis
- PMID: 28243383
- PMCID: PMC5326724
- DOI: 10.4184/asj.2017.11.1.150
Short Segment versus Long Segment Pedicle Screws Fixation in Management of Thoracolumbar Burst Fractures: Meta-Analysis
Abstract
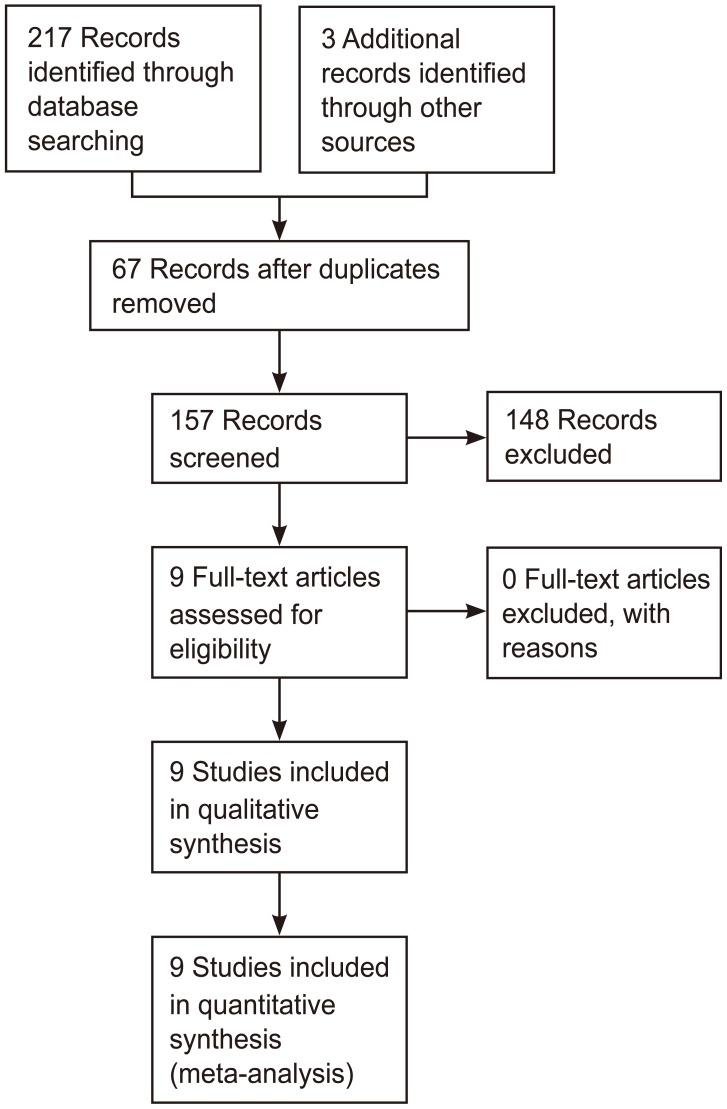
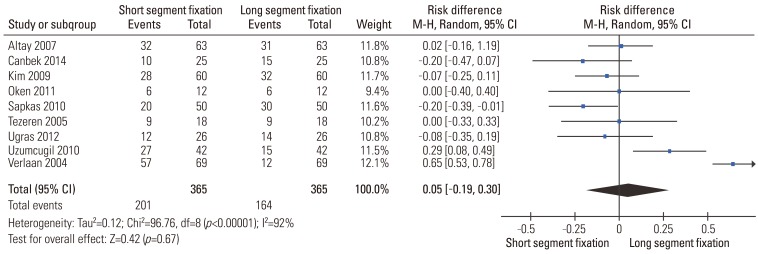
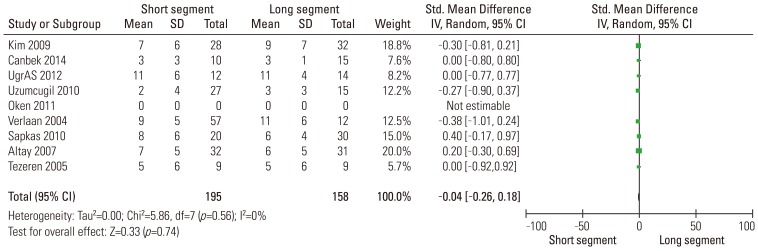
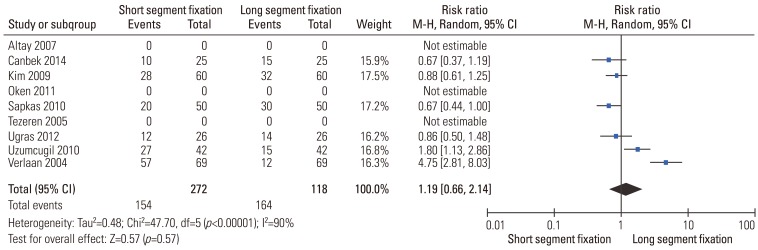
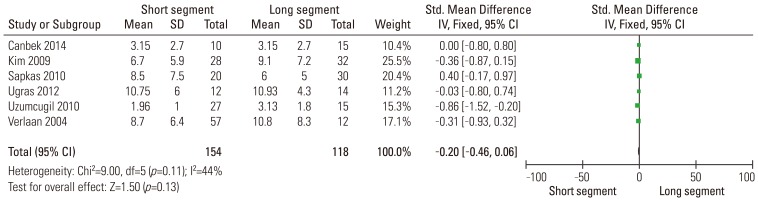
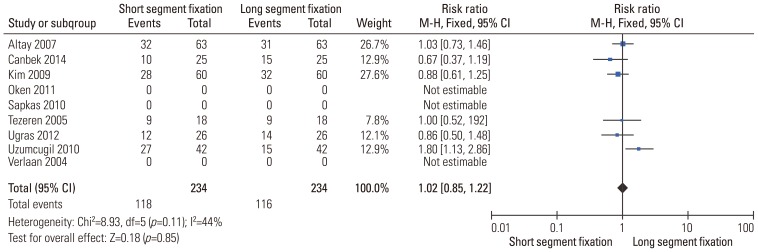
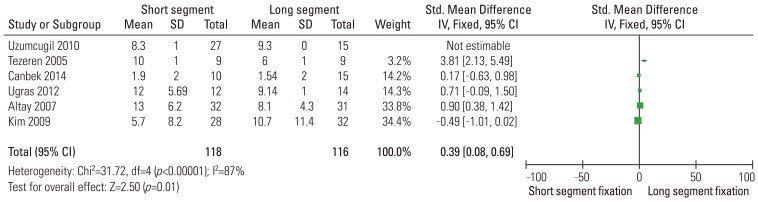
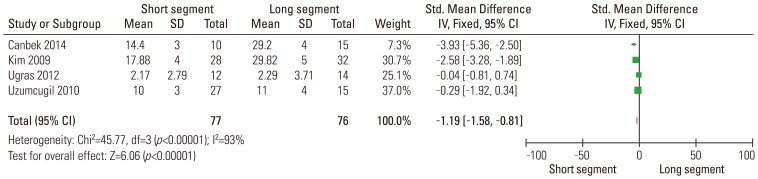
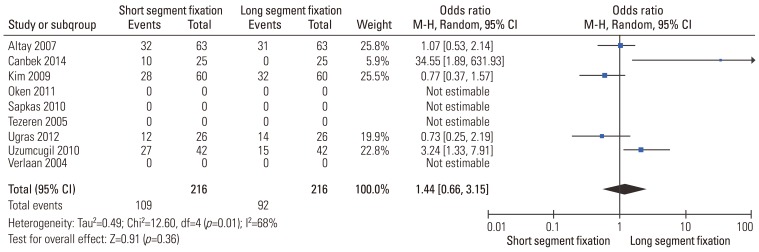
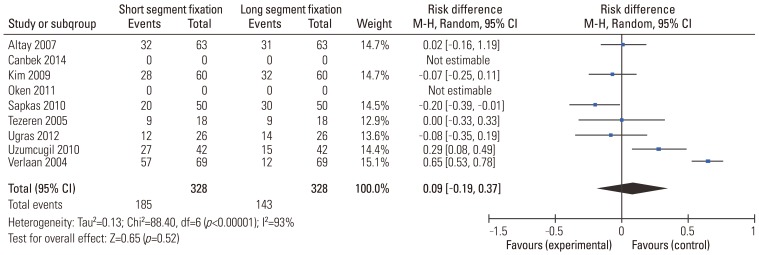
Posterior pedicle screw fixation has become a popular method for treating thoracolumbar burst fractures. However, it remains unclear whether additional fixation of more segments could improve clinical and radiological outcomes. This meta-analysis was performed to evaluate the effectiveness of fixation levels with pedicle screw fixation for thoracolumbar burst fractures. MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, Springer, and Google Scholar were searched for relevant randomized and quasirandomized controlled trials that compared the clinical and radiological efficacy of short versus long segment for thoracolumbar burst fractures managed by posterior pedicle screw fixation. Risk of bias in included studies was assessed using the Cochrane Risk of Bias tool. Based on predefined inclusion criteria, Nine eligible trials with a total of 365 patients were included in this meta-analysis. Results were expressed as risk difference for dichotomous outcomes and standard mean difference for continuous outcomes with 95% confidence interval. Baseline characteristics were similar between the short and long segment fixation groups. No significant difference was identified between the two groups regarding radiological outcome, functional outcome, neurologic improvement, and implant failure rate. The results of this meta-analysis suggested that extension of fixation was not necessary when thoracolumbar burst fracture was treated by posterior pedicle screw fixation. More randomized controlled trials with high quality are still needed in the future.
Keywords: Burst; Fixation; Long-segment; Pedicle screws; Short-segment; Spine; Thoracolumbar.
Conflict of interest statement
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Figures


References
-
- Dai LY, Yao WF, Cui YM, Zhou Q. Thoracolumbar fractures in patients with multiple injuries: diagnosis and treatment-a review of 147 cases. J Trauma. 2004;56:348–355. - PubMed
-
- Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine (Phila Pa 1976) 1983;8:817–831. - PubMed
-
- Jacobs RR, Asher MA, Snider RK. Thoracolumbar spinal injuries: a comparative study of recumbent and operative treatment in 100 patients. Spine (Phila Pa 1976) 1980;5:463–477. - PubMed
-
- Kaneda K, Taneichi H, Abumi K, Hashimoto T, Satoh S, Fujiya M. Anterior decompression and stabilization with the Kaneda device for thoracolumbar burst fractures associated with neurological deficits. J Bone Joint Surg Am. 1997;79:69–83. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
