

cEEG electrode-related pressure ulcers in acutely hospitalized patients
- PMID: 28243502
- PMCID: PMC5310208
- DOI: 10.1212/CPJ.0000000000000312
cEEG electrode-related pressure ulcers in acutely hospitalized patients
Abstract
Background: Pressure ulcers resulting from continuous EEG (cEEG) monitoring in hospitalized patients have gained attention as a preventable medical complication. We measured their incidence and risk factors.
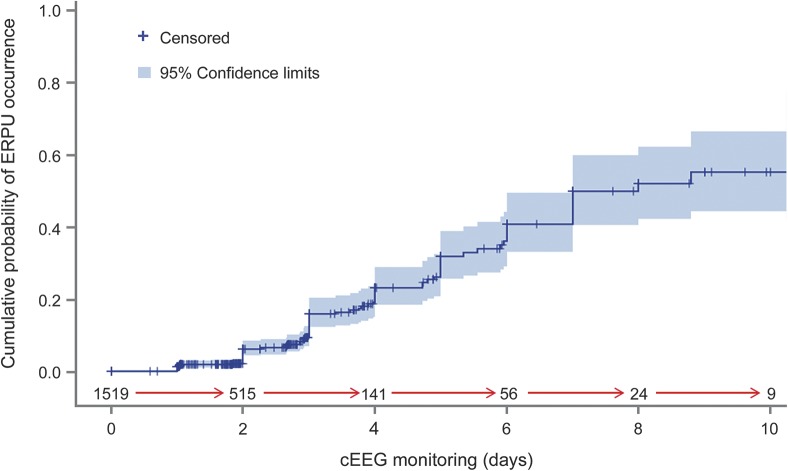
Methods: We performed an observational investigation of cEEG-electrode-related pressure ulcers (EERPU) among acutely ill patients over a 22-month period. Variables analyzed included age, sex, monitoring duration, hospital location, application methods, vasopressor usage, nutritional status, skin allergies, fever, and presence/severity of EERPU. We examined risk for pressure ulcers vs monitoring duration using Kaplan-Meyer survival analysis, and performed multivariate risk assessment using Cox proportional hazard model.
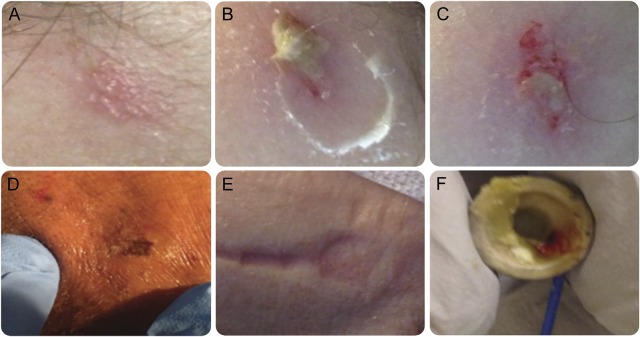
Results: Among 1,519 patients, EERPU occurred in 118 (7.8%). Most (n = 109, 92.3%) consisted of hyperemia only without skin breakdown. A major predictor was monitoring duration, with 3-, 5-, and 10-day risks of 16%, 32%, and 60%, respectively. Risk factors included older age (mean age 60.65 vs 50.3, p < 0.01), care in an intensive care unit (9.37% vs 5.32%, p < 0.01), lack of a head wrap (8.31% vs 27.3%, p = 0.02), use of vasopressors (16.7% vs 9.64%, p < 0.01), enteral feeding (11.7% vs 5.45%, p = 0.04), and fever (18.4% vs 9.3%, p < 0.01). Elderly patients (71-80 years) were at higher risk (hazard ratio 6.84 [1.95-24], p < 0.01), even after accounting for monitoring time and other pertinent variables in multivariate analysis.
Conclusions: EERPU are uncommon and generally mild. Elderly patients and those with more severe illness have higher risk of developing EERPU, and the risk increases as a function of monitoring duration.
Figures
References
-
- Claassen J, Mayer SA, Kowalski RG, Emerson RG, Hirsch LJ. Detection of electrographic seizures with continuous EEG monitoring in critically ill patients. Neurology 2004;62:1743–1748. - PubMed
-
- Friedman D, Claassen J, Hirsch LJ. Continuous electroencephalogram monitoring in the intensive care unit. Anesth Analg 2009;109:506–523. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources