

Joint Estimation of Cardiac Toxicity and Recurrence Risks After Comprehensive Nodal Photon Versus Proton Therapy for Breast Cancer
- PMID: 28244411
- PMCID: PMC5625081
- DOI: 10.1016/j.ijrobp.2016.12.008
Joint Estimation of Cardiac Toxicity and Recurrence Risks After Comprehensive Nodal Photon Versus Proton Therapy for Breast Cancer
Abstract
Purpose: The study aims to perform joint estimation of the risk of recurrence caused by inadequate radiation dose coverage of lymph node targets and the risk of cardiac toxicity caused by radiation exposure to the heart. Delivered photon plans are compared with realistic proton plans, thereby providing evidence-based estimates of the heterogeneity of treatment effects in consecutive cases for the 2 radiation treatment modalities.
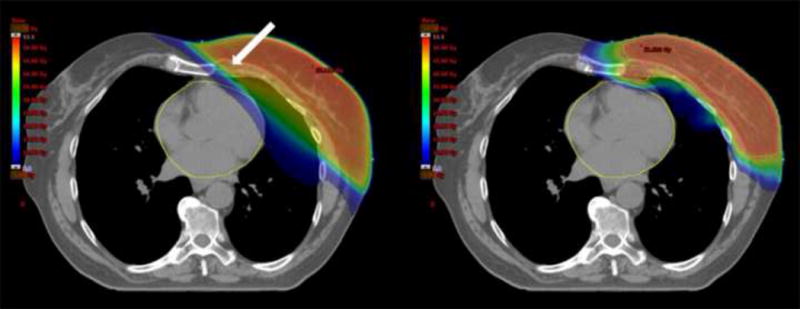
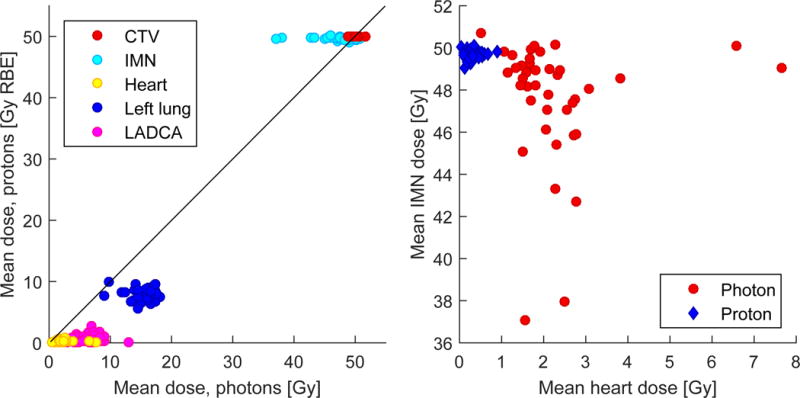
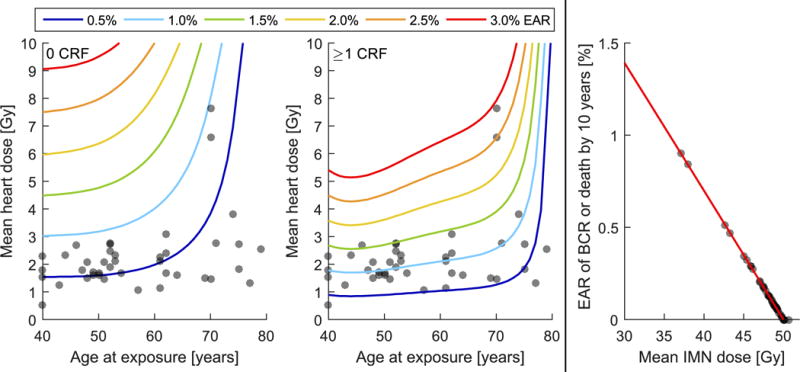
Methods and materials: Forty-one patients referred for postlumpectomy comprehensive nodal photon irradiation for left-sided breast cancer were included. Comparative proton plans were optimized by a spot scanning technique with single-field optimization from 2 en face beams. Cardiotoxicity risk was estimated with the model of Darby et al, and risk of recurrence following a compromise of lymph node coverage was estimated by a linear dose-response model fitted to the recurrence data from the recently published EORTC (European Organisation for Research and Treatment of Cancer) 22922/10925 and NCIC-CTG (National Cancer Institute of Canada Clinical Trials Group) MA.20 randomized controlled trials.
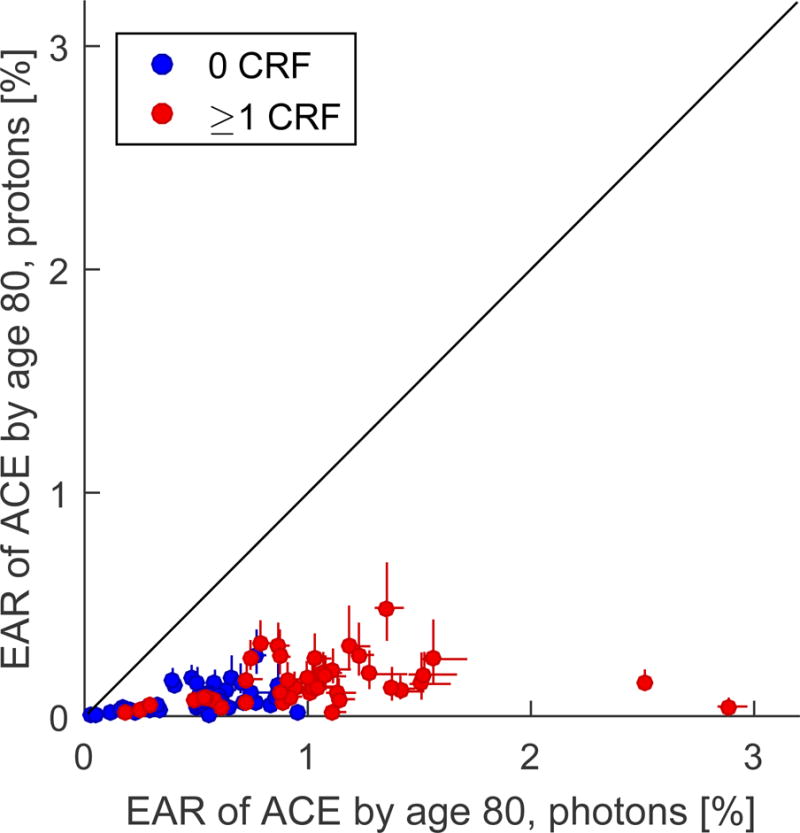
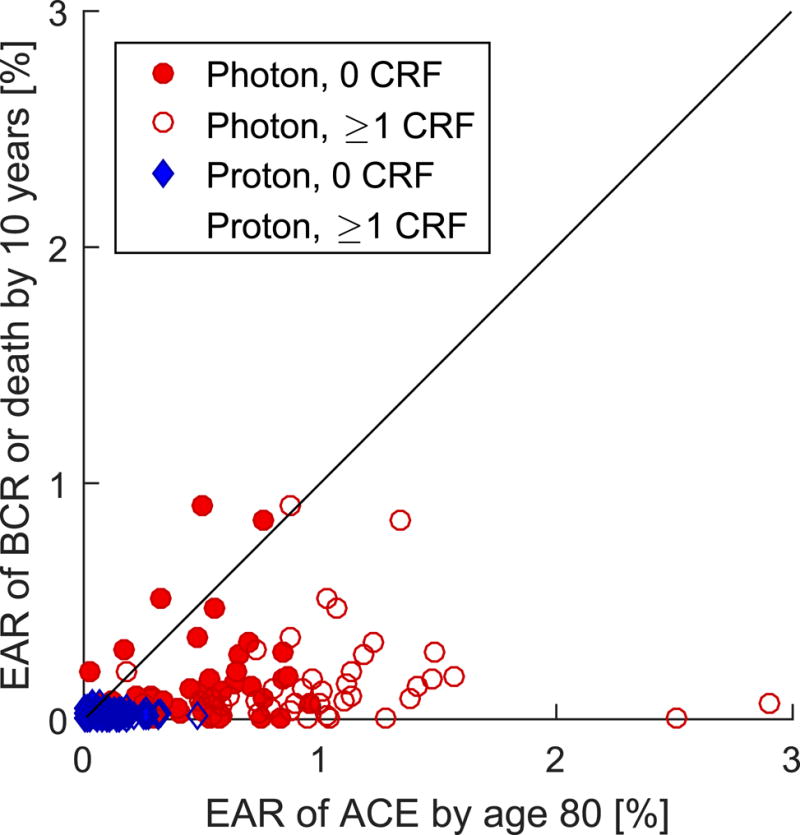
Results: Excess absolute risk of cardiac morbidity was small with photon therapy at an attained age of 80 years, with median values of 1.0% (range, 0.2%-2.9%) and 0.5% (range, 0.03%-1.0%) with and without cardiac risk factors, respectively, but even lower with proton therapy (0.13% [range, 0.02%-0.5%] and 0.06% [range, 0.004%-0.3%], respectively). The median estimated excess absolute risk of breast cancer recurrence after 10 years was 0.10% (range, 0.0%-0.9%) with photons and 0.02% (range, 0.0%-0.07%) with protons. The association between age of the patient and benefit from proton therapy was weak, almost non-existing (Spearman rank correlations of -0.15 and -0.30 with and without cardiac risk factors, respectively).
Conclusions: Modern photon therapy yields limited risk of cardiac toxicity in most patients, but proton therapy can reduce the predicted risk of cardiac toxicity by up to 2.9% and the risk of breast cancer recurrence by 0.9% in individual patients. Predicted benefit correlates weakly with age. Combined assessment of the risk from cardiac exposure and inadequate target coverage is desirable for rational consideration of competing photon and proton therapy plans.
Copyright © 2016. Published by Elsevier Inc.
Conflict of interest statement
Conflict of interest: IRV and MCA receive grants and educational fees from Varian Medical Systems.
Figures
References
-
- Poortmans PM, Collette S, Kirkove C, et al. Internal mammary and medial supraclavicular irradiation in breast cancer. N Engl J Med. 2015;373:317–27. - PubMed
-
- Thorsen LBJ, Offersen BV, Danø H, et al. DBCG-IMN: A Population-Based Cohort Study on the Effect of Internal Mammary Node Irradiation in Early Node-Positive Breast Cancer. J Clin Oncol. 2016;34:314–20. - PubMed
-
- Darby SC, Ewertz M, McGale P, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368:987–98. - PubMed
-
- Nissen HD, Appelt AL. Improved heart, lung and target dose with deep inspiration breath hold in a large clinical series of breast cancer patients. Radiother Oncol. 2013;106:28–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
