

Effectiveness and usage of a decision support system to improve stroke prevention in general practice: A cluster randomized controlled trial
- PMID: 28245247
- PMCID: PMC5330455
- DOI: 10.1371/journal.pone.0170974
Effectiveness and usage of a decision support system to improve stroke prevention in general practice: A cluster randomized controlled trial
Abstract
Background: Adherence to guidelines pertaining to stroke prevention in patients with atrial fibrillation is poor. Decision support systems have shown promise in increasing guideline adherence.
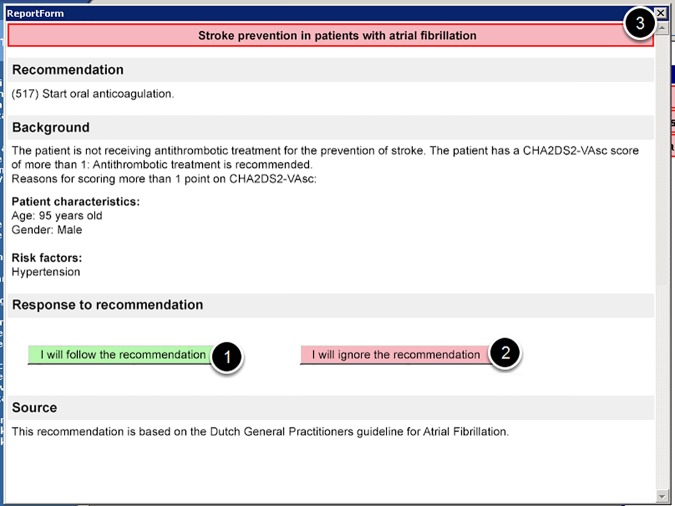
Aims: To improve guideline adherence with a non-obtrusive clinical decision support system integrated in the workflow. Secondly, we seek to capture reasons for guideline non-adherence.
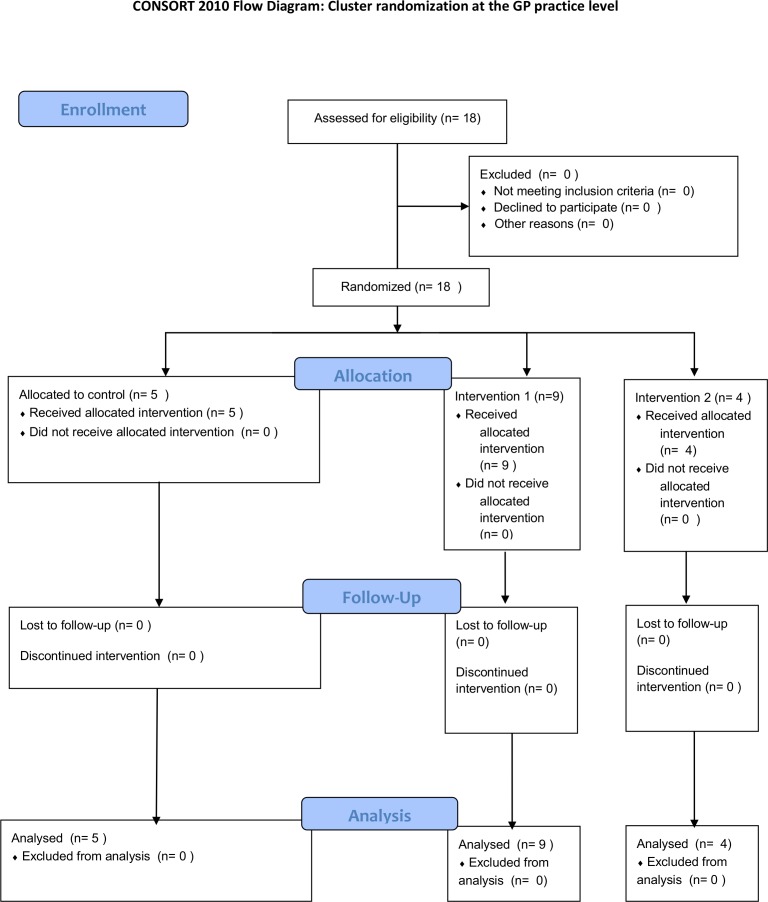
Design and setting: A cluster randomized controlled trial in Dutch general practices.
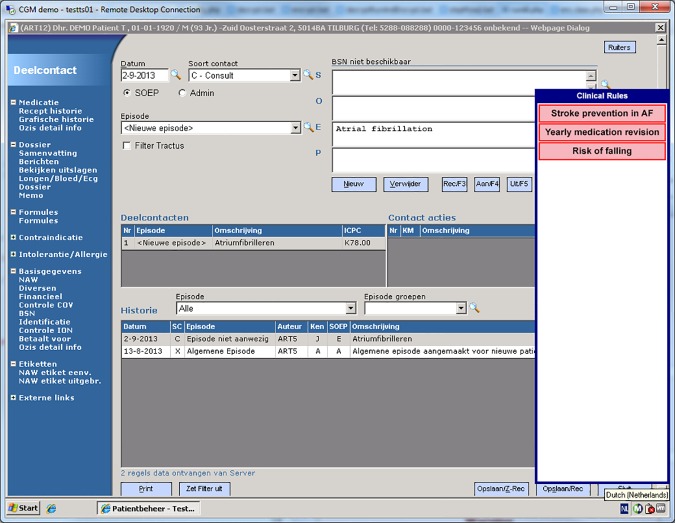
Method: A decision support system was developed that implemented properties positively associated with effectiveness: real-time, non-interruptive and based on data from electronic health records. Recommendations were based on the Dutch general practitioners guideline for atrial fibrillation that uses the CHA2DS2-VAsc for stroke risk stratification. Usage data and responses to the recommendations were logged. Effectiveness was measured as adherence to the guideline. We used a chi square to test for group differences and a mixed effects model to correct for clustering and baseline adherence.
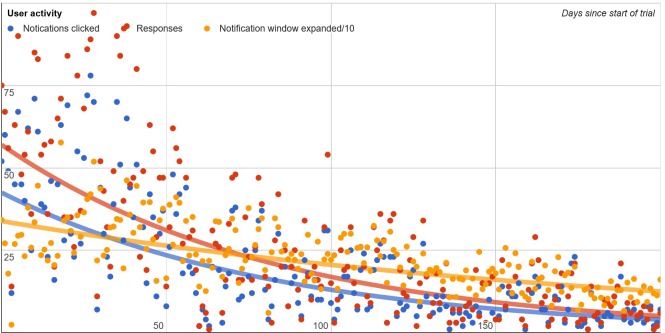
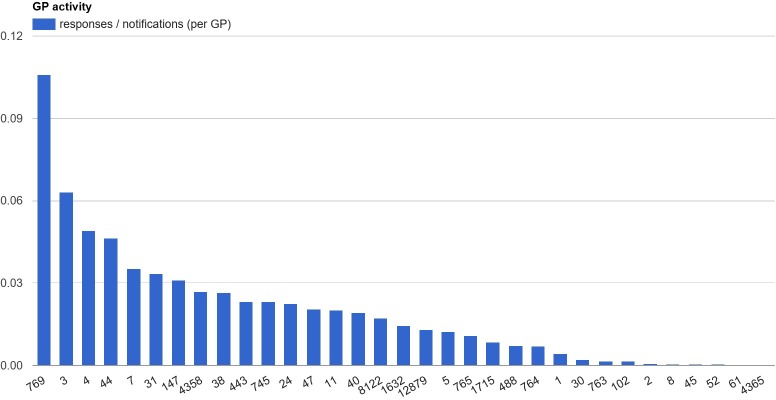
Results: Our analyses included 781 patients. Usage of the system was low (5%) and declined over time. In total, 76 notifications received a response: 58% dismissal and 42% acceptance. At the end of the study, both groups had improved, by 8% and 5% respectively. There was no statistically significant difference between groups (Control: 50%, Intervention: 55% P = 0.23). Clustered analysis revealed similar results. Only one usable reasons for non-adherence was captured.
Conclusion: Our study could not demonstrate the effectiveness of a decision support system in general practice, which was likely due to lack of use. Our findings should be used to develop next generation decision support systems that are effective in the challenging setting of general practice.
Conflict of interest statement
Figures
References
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22(8):983–8. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146(12):857–67. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
