

Vitamin A Supplementation Programs and Country-Level Evidence of Vitamin A Deficiency
- PMID: 28245571
- PMCID: PMC5372853
- DOI: 10.3390/nu9030190
Vitamin A Supplementation Programs and Country-Level Evidence of Vitamin A Deficiency
Abstract
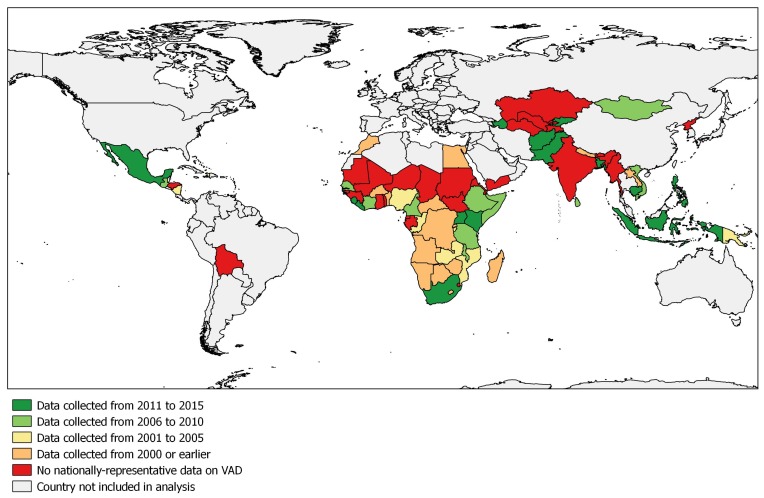
Vitamin A supplementation (VAS) programs targeted at children aged 6-59 months are implemented in many countries. By improving immune function, vitamin A (VA) reduces mortality associated with measles, diarrhea, and other illnesses. There is currently a debate regarding the relevance of VAS, but amidst the debate, researchers acknowledge that the majority of nationally-representative data on VA status is outdated. To address this data gap and contribute to the debate, we examined data from 82 countries implementing VAS programs, identified other VA programs, and assessed the recentness of national VA deficiency (VAD) data. We found that two-thirds of the countries explored either have no VAD data or data that were >10 years old (i.e., measured before 2006), which included twenty countries with VAS coverage ≥70%. Fifty-one VAS programs were implemented in parallel with at least one other VA intervention, and of these, 27 countries either had no VAD data or data collected in 2005 or earlier. To fill these gaps in VAD data, countries implementing VAS and other VA interventions should measure VA status in children at least every 10 years. At the same time, the coverage of VA interventions can also be measured. We identified three countries that have scaled down VAS, but given the lack of VA deficiency data, this would be a premature undertaking in most countries without appropriate status assessment. While the global debate about VAS is important, more attention should be directed towards individual countries where programmatic decisions are made.
Keywords: MNPs; biofortification; deficiency; fortification; programs; supplementation; vitamin A.
Conflict of interest statement
J.P.W., N.P. and F.R. are employees of GroundWork, a company providing technical support for the implementation of nutrition surveys. L.M.R. is an employee of the World Health Organization, a global UN agency that recommends that children 6–59 months of age in countries at risk of VAD should receive VAS every 4–6 months. E.M. is an employee of UNICEF, a UN agency that supports governments in the implementation of programs, including VAS programs. A.G. and R.D.W.K. are employees of Micronutrient Initiative and Helen Keller International, respectively, non-for-profit agencies that provide technical and/or financial support for the procurement of vitamin A capsules and implementation vitamin A supplementation programs. GSG is an employee of GAIN, a not-for-profit organization that supports national food fortification programs in countries where there is a demonstrated need and a food vehicle which can be fortified. S.A.T. is an employee of the University of Wisconsin-Madison and declares no conflict of interest. The authors alone are responsible for the views expressed in this publication and they do not represent the decisions, policies or views of the World Health Organization, UNICEF, Helen Keller International, the Micronutrient Initiative, GAIN, the University of Wisconsin-Madison, or GroundWork.
Figures
References
-
- World Health Organization . Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005. World Health Organization; Geneva, Switzerland: 2009. [(accessed on 17 February 2017)]. Available online: http://apps.who.int/iris/bitstream/10665/44110/1/9789241598019_eng.pdf.
-
- Stevens G.A., Bennett J.E., Hennocq Q., Lu Y., De-Regil L.M., Rogers L., Danaei G., Li G., White R.A., Flaxman S.R., et al. Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: A pooled analysis of population-based surveys. Lancet Glob. Health. 2015;3:e528–e536. doi: 10.1016/S2214-109X(15)00039-X. - DOI - PubMed
-
- Engle-Stone R., Haskell M.J., Nankap M., Ndjebayi A.O., Brown K.H. Breast milk retinol and plasma retinol-binding protein concentrations provide similar estimates of vitamin A deficiency prevalence and identify similar risk groups among women in Cameroon but breast milk retinol underestimates the prevalence of deficiency among young children. J. Nutr. 2014;144:209–217. - PubMed
-
- Alvarez J.O., Salazarlindo E., Kohatsu J., Miranda P., Stephensen C.B. Urinary-excretion of retinol in children with acute diarrhea. Am. J. Clin. Nutr. 1995;61:1273–1276. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
